

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The role of angiotensin receptor blockers (ARBs) in attenuating ischemia-reperfusion injury is not fully elucidated. It has been suggested that the myocardial protective effects of ARB against ischemia-reperfusion injury is mediated by activation of angiotensin II type 2 (AT2) receptors by angiotensin II, while the deleterious effects of AT1 receptors are blocked by the ARB (1, 2), leading to release of bradykinin with downstream activation of protein kinase C, nitric oxide synthase and eicosanoid release (2, 3, 4).
Fimasartan (BR-A-657-K, KANARB®, Boryung Pharmaceutical Co., Ltd, Seoul, Republic of Korea) is a new ARB developed for the first time in Korea. It is a selective blocker of AT1 receptor subtype and has shown rapid and potent antihypertensive effect in a number of clinical trials (5, 6, 7, 8). Furthermore, anti-atherosclerotic effects of fimasartan were demonstrated in animal studies (9, 10). However, the efficacy of fimarsartan in acute MI is not elucidated. The goal of the present study is, therefore, to evaluate the effect of fimasartan in a porcine model of acute myocardial infarction (MI).
MATERIALS AND METHODS
Induction of acute MI
This study was conducted on a total of 50 swine at the animal catheterization laboratory of Chonnam National University Hospital in Gwangju, Korea between May 2011 and June 2013. Landrace swine (20-25 kg) were provided and observed in the animal breeding house of Chonnam National University Medical Institute for 3-5 days before the experiment. All swine were given loading doses of aspirin (300 mg) and clopidogrel (300 mg) on the morning of the experiment, followed by aspirin 100 mg and clopidogrel 75 mg daily throughout the study period of 6 weeks. Experiment was done under anesthesia with zolazepam (2.5 mg/kg, intramuscular), tiletamine (2.5 mg/kg, intramuscular), xylazine (3 mg/kg, intramuscular), and azaperone (6 mg/kg, intramuscular). A 7F arterial sheath was placed in the left carotid artery under local anesthesia with 2% lidocaine. After infusion of 10,000 units of heparin, a 7F coronary artery guiding catheter was placed within the opening of the coronary artery and baseline coronary angiogram was obtained under the fluoroscopic guidance by mobile C-arm (Phillips BV-25 Gold). Acute MI model was induced with inflation of a balloon (3.0×20 mm, Terumo Co. Tokyo, Japan) just distal to the first diagonal branch or the septal branch. Complete occlusion was maintained by balloon dilatation (up to 8 atmospheres) for 50 min (Fig. 1). During the experiment oxygen and normal saline were supplied continuously and the anesthesia maintained with an additional administration of zolazepam (1.25 mg/kg, intravenous injection), tiletamine (1.25 mg/kg, intravenous injection), xylazine (1.5 mg/kg, intravenous injection), and azaperone (6 mg/kg, intramuscular injection). Continuous electrocardiographic monitoring was performed to confirm normal ST segment at baseline and ST elevation during the ischemic period and to monitor occurrence of cardiac arrhythmia. After induction of acute MI, each swine was closely observed for 1 hr for development of ventricular tachycardia or fibrillation, after which the swine was carried back to the breeding house and monitored until recovery.
Study groups and medications
The swine were randomly divided into 5 groups: group 1 (sham operation without induction of acute MI, n=10); group 2 (no ACEI or ARB post-MI, n=10); group 3 (perindopril 2 mg daily post-MI, n=10); group 4 (valsartan 40 mg daily post-MI, n=10); and group 5 (fimasartan 30 mg daily post-MI, n=10). Drug dosage was arbitrarily selected as half the initial dose in adult humans with hypertension. Study medications were administered orally 6-12 hr after the experiment and maintained for 4 weeks afterwards. Given the rapid growth of the animals (10-15 kg weight gain over a few weeks), the dose of each study medication was doubled after 2 weeks and maintained throughout the rest of the study period (Fig. 2).
Two-dimensional echocardiography
All swine underwent 2-dimensional transthoracic echocardiographic examination at baseline (before the procedure), 1 week, and 4 weeks after induction of acute MI (Fig. 2). Left ventricular ejection fraction (LVEF) and LV end-systolic volume (LVESV) and LV end-diastolic volume (LVEDV) were determined by modified biplane Simpson's rule in the 2- and 4-chamber views (11). Considering the rapid growth of the animal, LVESV and LVEDV were normalized to the animal's body surface area in order to more adequately present the data over time, as both volumes naturally increase with growth of the animal (12). A global diastolic function was assessed using transmitral inflow parameters: peak early (E) and peak late (A) velocities, E-wave deceleration time (DT) and E/A ratio. In addition, tissue Doppler imaging of mitral annular velocities (E', A') was measured. For the prediction of LV filling pressures, E/E' was calculated (13).
Tc-99m sestamibi myocardial perfusion SPECT
All swine underwent technetium (Tc)-99m sestamibi myocardial perfusion single photon emission computed tomography (SPECT) at resting state 3 times at baseline (before the procedure) and 1 week and 4 weeks after the procedure (Fig. 2 and 3). Resting ECG-gated Tc-99m sestamibi SPECT imaging was performed in concordance with standards of the American Society of Nuclear Cardiology (14). The swine were fasted overnight, Tc-99m sestamibi 111 MBq was injected intravenously at rest. Forty minutes after the injection, the planar and SPECT images were acquired in the supine position with ECG-gated technique using eight frames for a cardiac cycle. The SPECT data was acquired using a dual-headed SMV DST-XLi gamma camera (GE Medical systems, Milwaukee, WI, USA) with low-energy, all purpose (LEAP) collimator, setting the energy photo-peak at 140 keV with a 20% symmetric window and a 90° acquisition arc. The SPECT acquisition was undertaken in 16 steps (32 projections) and each step collect counts for 30 sec. Reconstruction of the images was performed by filtered back projection using butterworth filter. After reconstruction by filtered back projection using butterworth filter, transaxial slices along the vertical long axis, the horizontal long axis, and the short axis were generated.
F-18 FDG cardiac PET/CT
After Tc-99m sestamibi myocardial perfusion SPECT, F-18 fluorodeoxyglucose (FDG) cardiac positron emission tomography (PET)/computed tomography (CT) (FDG PET) was done (Fig. 2 and 3). Imaging was performed on a Discovery STE PET/CT system (GE medical systems, Milwaukee, WI, USA). Preparation was performed using simplified glucose/insulin loading (20 g of dextrose intravenously with simultaneous intravenous and subcutaneous insulin to adjust blood glucose to 5 mM/L) (15). PET/CT acquisitions for the heart were started at 40 min after the injection of 7.4 MBq per kilogram of body weight. CT images were acquired using parameters with a peak voltage of 140 keV, a tube current of 20 mA×16 sec, a rotation time of 1.0 sec, a field of view of 50 cm and a slice thickness of 3.27 mm. Immediately following the CT acquisition, the PET data were acquired in the same anatomic locations in the 2D mode with acquisition time of 15 min. The CT data were used for attenuation correction and the images were reconstructed using a conventional iterative algorithm (OSEM). A Xeleris workstation (GE medical systems) providing multiplanar reformatted images was used for image display and analysis.
SPECT, PET data analysis
Perfusion SPECT and FDG PET which were done on the same day were evaluated simultaneously on the consensus of 2 independent nuclear physicians. LVEF was derived from the ECG-gated images from perfusion SPECT (16). Static tomographic images and polar maps were normalized to their maximum and used for visual analysis of regional perfusion/metabolism patterns using the American Heart Association 17-segment model. Perfusion defect size was quantified on polar maps according to a method described earlier (17). Visual classification was done for normal, matched defect, or mismatched segments. Segments with decreased uptake on perfusion SPECT were visually defined as matched defect segments if FDG uptake was concordantly decreased on PET. Segments with decreased uptake on perfusion SPECT were defined as mismatched segments if FDG uptake was not concordantly decreased on PET. Perfusion defect assessment on SPECT was performed using an automated quantification of total perfusion defect that was calculated as the percentage of the total surface area of the LV below the predefined uniform average deviation threshold weighted on a pixel-by-pixel basis by the severity of perfusion on a scale from 0 to 4 using Quantitative Perfusion SPECT (QPS) software (Cedars Sinai, Los Angeles, CA, USA).
I-123 MIBG cardiac scintigraphy
Two weeks after cessation of medication, Iodine-123 (I-123) meta-iodobenzylguanidine (MIBG) scintigraphy was done by method described previously (18). I-123 MIBG 111 MBq was injected intravenously. After 15 min postinjection, imaging was acquired using a dual-headed SMV DST-XLi gamma camera (GE Medical systems) (Fig. 4). A 10-min planar image acquisition of the anterior thorax was performed at 15 min, followed immediately by SPECT image acquisition. These 2 procedures were later repeated starting at 3 hr 50 min post-injection (Fig. 4). All imaging was performed with low-energy/high resolution collimators, with the camera peaked at 159 keV with a symmetric 20% energy window. Planar images were acquired at 30- and 70-degree left anterior oblique views and anterior views in 128×128 matrix. SPECT images were obtained with a minimum of 60 projections (30 sec/stop) over a 180-degree arc. All SPECT images were stored in a 64×64 matrix, with the use of camera zoom factor as appropriate to achieve a nominal pixel size of 6.4 mm (range: 6.0 to 6.8 mm). The heart/mediastinum count (H/M) ratio was determined from the delayed anterior planar I-123 MIBG image. The heart region of interest (ROI) was drawn manually to include all visible ventricular activity. A square mediastinal ROI (7×7 pixels) was drawn in the upper mediastinum, using the apices of the lungs as anatomic landmarks. The H/M ratio was calculated as the ratio of the counts/pixel in the 2 ROIs. The heart/mediastinum count (H/M) ratio was determined from the delayed anterior planar I-123 MIBG image. The washout rate (WR) was calculated using the following formula: ([H/M]early - [H/M]late])/(H/M)early×100 (%).
Pathological examination of infarcted myocardium
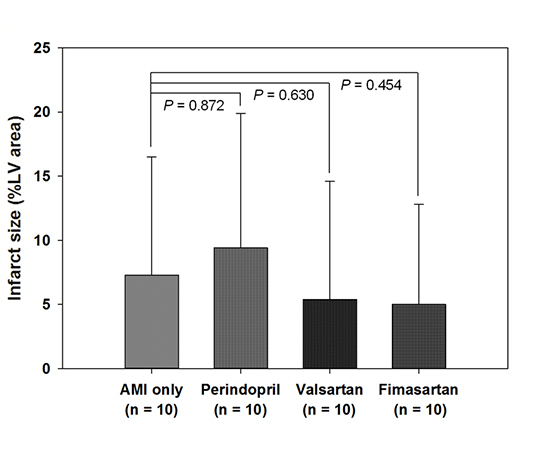
Six weeks later, a follow-up coronary angiography was performed according to the same protocol described above, after which the swine was sacrificed and the heart was extracted. The extracted heart was rinsed, and the myocardial sections including the left and right ventricle were obtained at 1-cm intervals using a microtome knife. The myocardial sections were incubated in 2,3,5-triphenyl tetrazolium chloride (TTC) solution until portions of viable myocardium turned brick red (Fig. 5). The specimens were reviewed by a cardiac pathologist for pathological changes in the infarcted myocardium. Histomorphometric infarct size was estimated on digital photographs of TTC staining by outlining the LV area and TTC negative infarct area. Infarct size was then expressed as % LV area (19).
Study endpoints
The primary end-point of the study was scintigraphic and pathologic myocardial infarct size. Secondary end-points were LV function and volumes on echocardiography and sympathetic nerve activity on MIBG scintigraphy.
Statistical analysis
All data were expressed as mean±standard deviation. Analysis was performed using SPSS statistical software, version 18.0 (SPSS Inc., Chicago, IL, USA). One-way ANOVA with Bonferroni's post hoc test for multiple comparisons was used to test for within-group and between-group comparisons. For all statistical analyses, the null hypothesis was rejected at the 95% confidence level, considering a P value <0.05 significant. To avoid type II errors (missing significant differences when the sample size is too small) we determined the required sample size for the present study using an approximation for α equal to 0.05 and power to 0.90 (20). Accordingly, 9 swine per group was the minimal sample size to detect differences of 10 mL in infarct size with a standard deviation of 5.1 based on our previous data recorded in identical experimental conditions (21). To compensate for possible dropouts, 10 animals were investigated in each group.
RESULTS
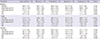
The results of SPECT and PET scans are described in Table 1. Heart rates were not different between the groups at baseline, 1 week, and 4 weeks. No significant difference was observed in SPECT perfusion defect extent, total perfusion defect, number of SPECT and PET defects across the groups at baseline, 1 week, and 4 weeks. The number of matched and mismatched segments between SPECT and PET at 1 week and 4 weeks was not different in groups 2 to 5, suggesting similar infarct size and viability. On MIBG scan at 6 weeks, groups 2 to 5 showed comparable H/M ratios for I-123 MIBG cardiac uptake at early (15 min) and late (3 hr 50 min) phases without significant difference in washout rate, indicating similar recovery of cardiac sympathetic nerve activity after acute MI (Table 2). Two-dimensional echocardiographic study revealed no difference in LV function and volumes at baseline (Table 3). At 1 week, LVEF was significantly lower in group 2 to 5 ranging from 29.3%±7.4% to 38.6%±14.7%, compared to sham control group (57.2%±7.1%) (P<0.001). At 4 weeks, however, LV systolic and diastolic functions improved to normal limits without between-group differences (Table 3). Pathologic analysis showed no significant difference in infarct size in groups 2 to 5 ranging from 5.0%±7.8% to 9.4%±10.5% of LV area (P=0.393) (Table 4, Fig. 6).
DISCUSSION
In the present study, use of fimasartan, a new ARB, after acute MI did not reduce infarct size in swine, compared to control groups. Myocardial viability, cardiac sympathetic nerve activity, LV function by SPECT, PET, MIBG scan and echocardiography as well as infarct size by SPECT, PET, and pathologic studies were not different between ACEI, ARB, and control groups.
Fimasartan (BR-A-657-K, KANARB®) is a new ARB developed for the first time in Korea. It is a selective blocker of AT1 receptor subtype and has shown rapid and potent antihypertensive effect in clinical trials (5, 6, 7, 8). Fimasartan was recently approved by Korea Food and Drug Administration for its safe and potent blood pressure lowering effect in patients with hypertension. However, there is a paucity of data on the efficacy of fimarsartan in atherosclerosis including acute MI. Lee et al. (9) reported that fimasartan attenuated atherosclerosis progression and reduced macrophage accumulation in the rabbit aortic plaques. Han et al. (10) observed that fimasartan pretreatment reduced ischemia/reperfusion injury and infarct size in rat hearts, indicating that fimasartan may prevent mitochondrial dysfunction and apoptosis accompanied by ischemia/reperfusion injury.
There have been inconsistent results concerning the effects of angiotensin inhibition on infarct size in animal models of acute MI (1, 2, 3, 17, 22, 23, 24, 25, 26, 27). In canine models, captopril administered after coronary occlusion reduced infarct size (17). In rat models of acute MI, losartan and ramiprilat protected the heart against ischemia/reperfusion injury independently of their hemodynamic effects but in a time-dependent manner (25). In contrast, several studies failed to demonstrate reduced infarct size with ramiprilat administered before, during, or after induction of myocardial ischemia in canine and mice hearts (26, 27, 28).
The failure to reduce infarct size in the present study utilizing porcine models may in part be explained from several perspectives. Firstly, angiotensin inhibition may exert time-dependent cardioprotective effects. Zhu et al. observed that pretreatment with losartan for 4 and 10 weeks, compared to pretreatment for 1 day or 1 week, before induction of acute MI reduced infarct size in a rat model of ischemia-reperfusion, suggesting time-dependent cardiovascular protective effects of losartan (29, 30). In the present study, ACEI and ARB were administered orally several hours after acute MI when the swine recovered from the anesthesia. This may have attenuated the effect of the study drugs in terms of protection from ischemia-reperfusion injury. Secondly, the doses of ACEI and ARB were arbitrarily chosen as half the initial dose in humans for essential hypertension and were doubled at 2 weeks considering the rapid growth of the swine. Due to lack of non-invasive methods available for serial blood pressure measurement in swine, we were unable to find the optimal tolerable doses that would maximize the beneficial effects of ACEI and ARB post-MI. On the contrary, the cardioprotective effect assessed by infarct size in the present study may have been confounded by the potent antihypertensive effect of the study drugs leading to increased infarct size compared to that of the AMI only group. However, since blood pressure measurements were not available in this study, it is difficult to provide evidence to support the impact of hemodynamic change on infarct size. Thirdly, most of the swine with persistent severe LV dysfunction after MI failed to survive and were dropped out early in the study period (overall mortality 45.6%) and the majority of the swine which completed the study showed preserved LV function. This again may have diluted cardioprotective effect of ACEI and ARB, which would play a major role in ischemic heart failure post-MI, leading to only modest infarct size ranging from 5%-9% of LV. Still, successful creation of a porcine acute MI model with severe LV dysfunction is a technical challenge with high periprocedural mortality. Finally, cardioprotective effect failed to be shown possibly due to the shorter duration of the study. The effect of blocking the renin-angiotensin-aldosterone system may take a longer period to be significant as shown in The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET) (31, 32). In addition, the favorable effect of this class of drugs in heart failure and renal protection supports that a longer duration may be needed in order to show its benefit. Nevertheless, the rapidly growing swine and the failure of the animal to survive the acute events as a result of severe heart failure reflects the difficulty of conducting this study. It remains to be further investigated whether cardiovascular protective benefits of ACEI and ARB including fimasartan are dependent on the time and duration of angiotensin inhibition and the drug doses before, during, or after induction of myocardial ischemia. In conclusion, the present study did not demonstrate infarct size reduction with use of a new ARB, fimasartan, as well as other ACEI and ARB in a porcine model of acute MI. The time- and dose-dependent cardiovascular protective effects of angiotensin inhibition needs to be determined.








 XML Download
XML Download