

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (PCa) is the most common male malignancy and the second most common cause of male cancer-related death (1). Today, in Korea, PCa is the fifth most common cancer in men, and its incidence is the most rapidly increasing of all cancers (2). In clinical practice, prostate-specific antigen (PSA) is one of the most important biomarkers for detecting PCa and a valid predictor for determining the presence of aggressive, potentially life-threatening PCa (3). There is strong evidence that the use of PSA for PCa screening, followed by treatment of PCa at an earlier stage, can reduce PCa-related mortality (4). Although a PSA cutoff level of 4.0 ng/mL has been used for prostate biopsy since the introduction of PSA-based screening, a considerable proportion of clinically significant PCa is detected at PSA levels lower than 4.0 ng/mL, indicating that lowering the PSA cutoff to 2.5 ng/mL would improve detection rates of PCa (5, 6). However, there has also been increasing concern regarding the over-diagnosis of cancers that would not have become life-threatening, leading to unnecessary treatment that may be associated with significant side effects (7, 8). There are still debates on optimal guidelines for the screening of PCa in the Korean population according to PSA level so as to identify only men with significant disease that would put them at risk if left undiagnosed.
Several previous studies have suggested the potential advantages of a lower PSA cutoff in an Asian population (9, 10). Kobayashi et al. (9) reported a PCa detection rate of 23.6% for Japanese men with PSA levels between 2.0 and 4.0 ng/mL, and one report (10) found a cancer detection rate of 26% in Korean men with PSA levels between 3.0 and 4.0 ng/mL. Furthermore, PCa in Korean men exhibits more intrinsically adverse pathologic characteristics and prognosis than that in American men, regardless of the initial serum PSA level or clinical stage at presentation, indicating that these Korean men underwent surgery at a more advanced stage (11, 12, 13). Therefore, novel and validated PCa screening and treatment strategies in Korea are unmet clinical needs. In the present study, we retrospectively compared clinicopathologic parameters and biochemical outcomes of PCa in men with PSA level in the range of 2.5 to 4.0 ng/mL, subdivided into 2.5-3.0 ng/mL and 3.0-4.0 ng/mL, with those of men with PSA level in the range of 4.0 to 10.0 ng/mL in order to determine the clinical implications of a lower cutoff range for prostate biopsy in Korean patients.
MATERIALS AND METHODS
Study subjects
A total of 1,617 Korean men who underwent radical prostatectomy
(RP) between 1995 and 2013 and who had PSA levels ranging from 2.5 to 10.0 ng/mL were enrolled in this study after exclusion of any patient who had history 5-alpha-reductase inhibitor use or received neo-adjuvant treatment before RP. All patients underwent digital rectal examination (DRE) following the collection of blood samples in order to determine total PSA level. Transrectal ultrasound (TRUS)-guided needle biopsy of the prostate was recommended for patients with a total PSA level of 2.5 ng/mL or higher, as was the additional use of findings by DRE and TRUS. Body mass index (BMI) was categorized according to the Asia-Pacific definition of obesity (<25 kg/m2 vs. ≥25 kg/m2). Prostate volumes were measured by TRUS or magnetic resonance imaging (MRI) and PSA density was calculated as preoperative PSA divided by prostate volume. All patients were preoperatively staged for metastases with a bone scan and an MRI scan or pelvic computed tomography (CT). For biopsy specimens, the Gleason score at biopsy (bGS) and number of positive biopsy cores were recorded.
Pathological examination
Prostatectomy specimens were reviewed with respect to pathologic GS (pGS), estimated total cancer volume, pathologic tumor stage, and surgical margin status. Total cancer volume was defined as the sum of the volumes of individual cancer foci. The key pathologic parameters considered as diagnostic of organ confinement status were extraprostatic extension (EPE), seminal vesicle invasion (SVI), and lymph node involvement (LNI), and pathologic organ-confined disease (OCD) was defined as pT2Nx-N0 PCa. We deemed men with a pGS <8 or pathologic stage ≤pT3a PCa at RP to have 'favorable' disease and those with pGS 8-10 and pT3b or N1 disease to have 'unfavorable' pathological findings. Insignificant cancer was also based on data from the European Randomized Study of Screening for Prostate Cancer, in which insignificant cancer was defined as a total tumor volume <2.5 mL with pGS ≤6 and pT2 stage (14). The follow-up schedule after RP involved a PSA assay every three months for the first two years, every six months for the following three years, and annually thereafter. Biochemical recurrence (BCR) was defined as the first occurrence of two consecutive PSA level increases >0.2 ng/mL at least three months after RP.
Statistical analysis
Qualitative data were tested using the chi-square test or Fisher's exact test as appropriate, and continuous data were evaluated using Student's t-test. The survival time analysis of BCR-free survival (BFS) was performed by Kaplan-Meier analysis, and differences were tested for statistical significance with the log-rank test. The influence of various parameters was analyzed with various multivariate Cox proportional hazards regression analyses to identify independent prognostic factors of BFS. All P values were two-sided, and a P<0.05 was considered statistically significant. All data analyses were performed with SPSS statistical software (Version 19.0, Chicago, IL, USA).
RESULTS
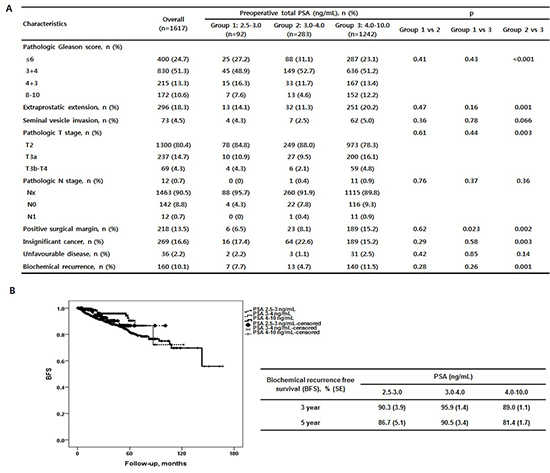
Patients were stratified by PSA level into three groups: group 1 (very low, 2.5-3.0 ng/mL), group 2 (low, 3.0-4.0 ng/mL), and group 3 (intermediate, 4.0-10.0 ng/mL). Of a total of 1,617 patients that met the criteria for study participation, group 1 contained 92 (5.7%), group 2 contained 283 (17.5%), and group 3 contained 1,242 (76.8%) patients. The patient preoperative demographics and clinical characteristics are presented in Table 1. The patients in group 1 (64 yr) were younger than those in group 2 (65 yr, P=0.04), but there was no difference in age between group 1 and group 3 (P=0.18). Prostate-specific antigen density (PSAD) was significantly lower in group 1 (0.10 ng/mL2) than in group 3 (0.22 ng/mL2, P<0.001) but was comparable between group 1 and group 2 (0.13 ng/mL2, P=0.08). The pathologic findings of the needle biopsy samples revealed no significant differences between group 1 and group 2, including percentage of patients with three or more positive cores (P=0.53) or the proportion of bGS (P=0.35). Interestingly, while the percentage of patients with bGS 7 or higher was significantly lower in group 2 than in group 3 (38.2% vs. 58.4%, P=0.002), the proportion of patients with higher bGS (≥7) was similar in group 1 and group 3 (P=0.59). In addition, the percentage of patients clinically presenting non-organ confined disease (NOCD) did not differ among the three groups (26.1%, 23.3%, and 28.9%, all P>0.05).
The pathologic characteristics of prostatectomy specimens and BCR rates are summarized in Table 2. No meaningful differences were noted between group 1 and group 2 with regard to the pathologic features of the prostatectomy specimens, including total cancer volume, distribution of pGS, pathological stage, percentage of positive surgical margin (PSM), percentage of insignificant PCa, or percentage of unfavorable disease (Table 2). Interestingly, group 1 and group 3 had no statistically significant differences in pGS (P=0.43), pathologic T (P=0.44) and N stage (P=0.37), or rates of insignificant (P=0.58) or unfavorable cancer (P=0.85), but statistically significant differences were found in total cancer volume (2.5 mL vs. 4.3 mL, P<0.001) and PSM rate (6.5% vs. 15.2%, P=0.023). In total, 23.9% of patients (n=22) had pGS of 4+3 or higher, 15.2% (n=14) had pathological stage ≥T3, and 82.6% (n=16) had significant PCa with PSA in the range of 2.5-3.0 ng/mL (i.e., group 1). During a median follow-up of 33 months, a total of 160 patients (10.1%) experienced BCR events, and the BCR rate was not significantly different between group 1 and group 2 (7.7% vs. 4.7%, P=0.28) or between group 1 and group 3 (7.7% vs. 11.5%, P=0.26), although group 2 had a significantly lower BCR rate than did group 3 (P<0.001). The five-year BFS rate was 86.7% in group 1, 90.5% in group 2, and 81.4% in group 3 (Fig. 1), suggesting that biochemical outcome in group 1 was not better than that in group 2 (Log rank, P=0.38).
The distributions of bGS/pGS and disease status after RP in the subpopulation with bGS ≤4+3 and of clinical organ confined disease (OCD) status are shown in Table 3 for the assessment of the influence of stratified PSA on upgrading or upstaging. Statistically significant differences in the percentages of upgrading and upstaging were not found among the three subgroups of PSA level (P=0.18 and P=0.40, respectively). Interestingly, within the PSA range of 2.5-3.0 ng/mL, 30.7% of patients were upgraded from bGS 6 to pGS >6, and 14.7% were upstaged from clinically OCD to NOCD on final pathology in our series. The corresponding values of those parameters at the PSA range of 3.0-4.0 ng/mL were 33.9% and 8.8%, respectively, while those in the PSA range of 4.0-10.0 ng/mL were 32.8% and 13.8%.
Table 4 shows the multivariate analysis of variables that could potentially predict PSA failure. After adjusting for age (<70 yr vs. ≥70 yr), PSAD (<0.2 ng/mL2 vs. ≥0.2 ng/mL2), pGS (6 vs. 3+4 vs. 4+3 vs. 8-10), pathologic stage (OCD vs. NOCD) and surgical margin status (negative vs. positive), PSA subgrouping was not predictive of BCR (PSA 3.0-4.0 ng/mL, P=0.27; PSA 4.0-10.0 ng/mL, P=0.90). Higher pGS (3+4, hazard ratio [HR], 1.85, P=0.02; 4+3, HR, 3.82, P<0.001; 8-10, HR, 7.40, P<0.001) and PSM (HR, 2.44, P<0.001) were significantly associated with BCR.
DISCUSSION
Given the well-accepted ethnicity-based differences in PCa characteristics between Western and Korean populations (9, 11, 12), PCa screening protocols validated in Western institutions might not be applicable in Korean men. In a recent study analyzing 6,651 Korean men, the optimal PSA value to distinguish the risk of PCa was 2.0 ng/mL for 50- to 69-yr-olds (15). However, in current practice patterns of Korean urology, the rates of prostate biopsy were 7.1%, 26.3%, 54.2%, and 64.3% for PSA levels of 2.5-3.0, 3.0-4.0, 4.0-10.0, and >10.0 ng/mL, respectively; and the PCa detection rates were 16.0%, 22.2%, 20.2%, and 59.6% (16).
Most of the PCa detected in the low PSA range was clinically significant (9, 17), and there were no differences in pathologic stage or Gleason pattern between patients with low PSA level (2.0-4.0 ng/mL) and high PSA level (4.0-10.0 ng/mL) (18). Importantly, most of these cancers are clinically significant, with more than 80% of them being organ-confined and thus candidates for curative treatments (19). In agreement with previous studies, our study demonstrated comparable pathological characteristics, biochemical outcomes, and rates of upgrading/upstaging among the three groups. Furthermore, the incidence of clinically significant PCa was 82.6% for PSA levels of 2.5-3.0 ng/mL, 77.4% for PSA levels of 3.0-4.0 ng/mL, and 84.8% for PSA levels of 4.0-10.0 ng/mL. Taken together, these data suggest that a lower PSA threshold of 2.5 ng/mL may be a more appropriate cutoff point that should be considered for prostate biopsy in the Korean population.
Pretreatment variables, most commonly PSA, clinical stage and bGS, have been used to predict the probability of upgrading at surgery, extent of disease at surgery, and BCR risk after treatment (20). Among preclinical factors, GS is usually the preeminent factor that is considered in counseling patients about treatment options (21). The discrepancy between the bGS and the pGS often results in improper assessment of the disease, consequently influencing prognosis and outcome (22). As it has already been shown that upgrading after prostate biopsy is a frequent occurrence, we studied whether there was a difference in the amount of upgrading among the three PSA groups. In our sub-analysis, patients in the PSA ranges of 2.5-3.0, 3.0-4.0, and 4.0-10.0 ng/mL were upgraded from bGS 6 to pGS >6 with incidences of 30.7%, 33.9%, and 32.8%, respectively, revealing no distinct differences. In addition, the proportions of patients with pGS ≥4+3, a significant predictor of BCR, were 23.9%, 16.3%, and 25.6%, respectively, in the three groups.
The PSA test is not reliably able to distinguish indolent from aggressive cancers (23). The amount of PSA produced per unit tumor volume was shown to decrease with increasing GS, thereby diminishing the predictive value of PSA (24). Controversies regarding the impact of PSA in PCa prognosis and outcome after RP have motivated several investigations and comparative analyses of PSA-based parameters (PSAD, PSA-doubling time, PSA velocity, and PSA slope) as potential predictors of adverse pathology, metastatic progression, and cancer-specific mortality (25). Among alternative indicators, PSAD has been promoted as a more specific indicator of PCa risk in patients with a PSA level <10 ng/mL and as a strong predictor of adverse pathological features and BCR after RP (26), although PSAD was not significantly associated with BCR in the present study. Additionally, age-specific reference ranges for PSA are widely used in the USA and European countries (5). Patients aged ≥70 yr were shown to have biologically more aggressive and locally advanced tumors significantly more often than did those aged <70 yr (27); similarly, we found old age (≥70 yr) to be an independent predictor of BCR. Accordingly, optimal PSAD or age-specific references for Korean men as critical determinants of prostate biopsy should be established and validated based on multi-center and large cohort studies.
We acknowledge that the present study has some limitations. First, our study was carried out retrospectively, and the data analyzed were from selected patients who underwent RP at a single institution, indicating an inherent selection bias. However, RP is necessary to confirm the pathological characteristics of insignificant prostate cancer, so selection bias may be unavoidable. Second, we focused primarily on pathological findings and BCR but did not assess prostate cancer-specific mortality, which might be a more important issue than adverse pathological characteristics. As advanced pathological stage or high-grade prostate cancer does not always correlate with long-term prognosis, the true clinical impact of the tumors in this current cohort remains unknown at present.
Collectively, no statistically significant difference was found in adverse pathological findings, including NOCD, higher GS and positive surgical margins and BCR when the PSA range of 2.5 to 3.0 ng/mL was compared with 3.0 to 4.0 or 4.0 to 10.0 ng/mL in Korean patients. Furthermore, within the population with PSA lower that 10 ng/mL, sub-stratification of PSA was not significant predictor for adverse pathological features and prognosis. Taken together, these results suggest that a lower PSA level should be considered as an indication for prostate biopsy in the Korean population.s


 XML Download
XML Download