

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A urethral stricture is a narrowing of the urethra caused by injury or disease such as urinary tract infections or other forms of urethritis, which sometimes makes it difficult to urinate (1). Functional urethral reconstruction depends on both the surgical techniques and materials used (2). Numerous urethral reconstruction materials have been described, but completely satisfactory ones remain to be found. Previous research has demonstrated that collagen-based materials, such as the small intestine, have potential regenerative capability (3) but have not achieved complete success owing to insufficient incorporation with the host urethra (4). Such inadequate incorporation can cause progressive scarring with stricture, contraction, diverticulum, and fistula formation (4).
Recently, bladder submucosa matrix (BSM), a collagen-based, nonimmunogenic, xenogenic material harvested from the submucosal layer of porcine bladders, has shown progress in preclinical and clinical applications for the reconstruction of numerous body structures (5). For example, urethra, ureter, and urinary bladder reconstruction using BSM showed evidence of reconstitution with innervated smooth muscle formation (6, 7, 8, 9, 10). However, BSM alone was not sufficient for complete tissue regeneration, despite direct in vivo placement by the cell-unseeded technique (11). An implanted BSM scaffold without cells showed contraction over time in an in vivo study (10). However, a cell-seeded BSM scaffold did not show the same phenomenon (10). Nevertheless, the cell-seeded method showed effective tissue reconstruction capability, but the cell processing procedures, such as cell harvest, proliferation and expansion, were time- and cost-depleting.
To overcome the weaknesses of these two techniques, we developed a tissue-embedded BSM graft. This method can avoid cell culture procedures, be used for direct in vivo placement, and increase incorporation between the graft and host tissue sufficiently. To increase graft incorporation into host tissue, autologous tissue was transferred into the damaged area, which was expected to reduce the risk of infection and rejection. However, autologous tissue may not be able to cover the entire recipient area owing to the limitation of the donor site, thus partial autologous tissue embedding on the scaffold was selected. Therefore, the objective of this study was to evaluate the reconstructive properties of a combined graft comprising acellular BSM and autologous urethral tissue for urethral reconstruction in a rabbit model.
MATERIALS AND METHODS
Preparation of acellular matrix
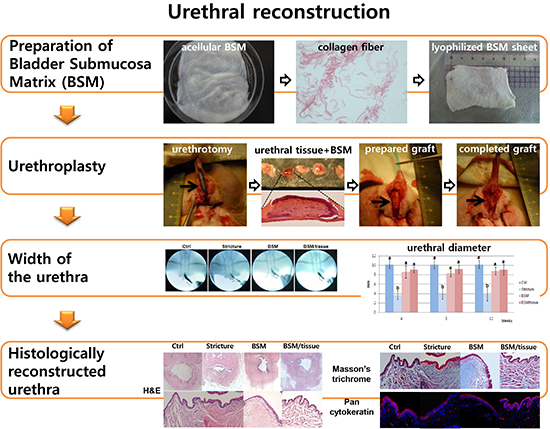
The mucosa of the porcine bladder was removed by surgical delamination. The dissected tissue was cross-sectioned and BSM was confirmed by hematoxylin and eosin (H&E) staining. The BSM was rinsed with water in a stirring flask (200 rpm) for 2 days at 4℃, treated with 0.03% trypsin for 1 hr, and finally treated with Triton X-100 (0.5%) and ammonium hydroxide (0.05%) in distilled water for 72 hr at 4℃. The solution was changed daily. After this procedure, a small piece of tissue was sampled for histology to confirm the levels of decellularization. The tissue was washed with distilled water for 2 days at 4℃, and then frozen, lyophilized, and stored at -80℃ before use (Fig. 1) (12).
Generation of a urethral stricture model and urethroplasty
A total of 20 male New Zealand white rabbits (Hyochang Science, Daegu, Korea) weighing 2.5 to 3.5 kg were assigned to four experimental groups (n=5 per group): control (sham), stricture (simple urethrotomy), BSM (onlay urethroplasty with an acellular BSM scaffold graft), and BSM/tissue (onlay urethroplasty with a graft composed of autologous urethral tissue [3×3 mm2 biopsy] and an acellular BSM scaffold).
Following a 12-hr fast, 15 rabbits were anesthetized by intramuscular injection of 3 mL of Zoletil (Virbac Animal Health, Milperra, NSW, Australia) and 1 mL of Rompun (Bayer, Leverkusen, Germany). Suprapubic cystostomy using a 6F pigtail catheter (Cook Medical, Bloomington, IN, USA) was performed to prevent urinary retention. A 5F catheter was inserted into the urethra. The anterior urethra was prepared and a ventral portion with a width of 5 mm and length of 20 mm including urethral muscle and endothelial tissues was excised to create a long-segment urethral stricture (Fig. 2A). The urethral defect was then primarily sutured (13). One month after generation of the urethral stricture, the 10 rabbits in the graft groups underwent urethroplasty. For the scaffold/tissue group, healthy urethral muscle and endothelial tissues (3×3 mm2) which were surgically excised from normal urethra located at the more proximal site of narrowed urethra were minced, placed onto the BSM graft (5×25 mm2), and fixed with 20 µL of fibrin glue (Greenplast, Greencross, Yongin, Korea) (Fig. 2B). The graft was meticulously mobilized (Fig. 2C) into the injured urethra, and interposed and anastomosed to the urethral defect using 6-0 vicryl (Ethicon, Somerville, NJ, USA) sutures (Fig. 2D). The scaffold group was treated with a BSM graft (5×25 mm2) in the same manner. Each end of the suture line was marked with a non-absorbable suture for future reference. The wound was then closed in layers with 5-0 vicryl (Ethicon) sutures. Urinary diversion was accomplished with a urethral catheter (Foley Balloon Catheter, Sewoon Medical, Cheonan, Korea) sewn to the external urethral meatus. A dual Elizabethan collar modification was used to prevent the animals from chewing their catheters. Cefazolin (Chongkundang, Seoul, Korea) was administered to all rabbits for a total of 7 days. The urethral catheter was removed from all rabbits 7 days postoperatively.
Retrograde urethrography
All animals underwent retrograde urethrography performed using the following protocol at 4, 8, and 12 weeks after surgery. Following general anesthesia, a 6F Foley catheter (Sewoon Medical, Cheonan, Korea) was secured in the distal urethral meatus. Renografin-76 (10 to 15 mL) was injected and real-time fluoroscopy (Philips Electronics, Eindhoven, Netherland) was used to obtain static images to document the urethral shape. The mean width of the operated urethra was measured from each radiographic image when the urethra was fully dilated.
Histologic and immunohistochemical analysis
Animals were sacrificed 12 weeks after the surgery, and the urethras were excised between the distal and proximal marking sutures. Tissue specimens were prepared for routine staining by hematoxylin and eosin (H&E), Masson's trichrome, and immunohistochemical (IHC) staining with a pancytokeratin antibody to identify urothelial regeneration. The specimens were fixed in 10% neutral buffered formalin for 24 hr and the paraffin-embedded specimens were sectioned at 4- to 6-µm thicknesses. Masson's trichrome staining was used to determine the distribution of muscle, keratin, and collagen. For pancytokeratin IHC staining, the paraffin sections were rehydrated, endogenous peroxidase was blocked with 0.3% hydrogen peroxide, and nonspecific protein was masked with 3% normal horse serum. The sections were incubated for 1 hr with primary antibody (1:100; Sigma Aldrich, St. Louis, MO, USA). After washing, the sections were immunostained using the avidinbiotin-peroxidase method and Elite ABC kit (Vector Laboratories, Burlingame, CA, USA) and counterstained with hematoxylin. As a negative control, the sections were stained without exposure to the primary antibody.
Statistical analysis
The width of the operated urethra among the control, stricture, and graft groups on retrograde urethrograms was measured at 4, 8, and 12 weeks postoperatively. The data are presented as the mean±standard deviation (SD). Statistical analysis was performed using Student's t-test or one-way analysis of variance. P<0.05 was considered statistically significant. When the P value was significant on analysis of variance, Tukey's post hoc comparison was used.
RESULTS
The mean operative time for generation of the long-segment urethral stricture and urethroplasty was 16 (range, 15 to 21) min and 31 (range, 25 to 37) min, respectively. No technical problems occurred during the surgeries. All animals survived for their intended survival period without any evidence of postoperative infection or voiding difficulties. All rabbits in the urethroplasty group had a good appetite and weight gain. No urethral fistula or stricture recurrence was observed in the urethroplasty group during the study period.
Retrograde urethrographic findings
The width of the penile urethra was measured by urethrograms at 4, 8, and 12 weeks postoperatively (Fig. 3A). The control urethrography showed a wide urethral caliber. Both graft groups showed a similar width to those of the normal group, and the stricture group revealed stenosis. Although the difference in the width of the BSM and BSM/tissue graft urethroplasty groups was not statistically significant, the BSM/tissue graft group showed an approximately 0.567-mm wider diameter (Fig. 3B).
Histologic and IHC findings
After the retrograde urethrogram at week 12, all rabbits were sacrificed, and the entire urethra was excised. The non-absorbable reference sutures were easily distinguishable on macroscopic inspection. At low magnification, H&E-stained cross-sections of the urethra of the control and graft groups revealed the presence of thick circular smooth muscle and a similar area of urethral lumen (Fig. 4A, C, D), whereas the stricture group showed loose muscle layers and a narrow lumen (Fig. 4B). In all cases in which grafts were surgically placed in the urethras, a diverticulum or fistula did not form in the graft area and the urethral luminal area was enlarged. Microscopically, the junction of the graft and normal urethra was not identifiable in both graft groups, indicating that the grafts were replaced by new tissue formation (Fig. 4C, D). At high magnification, the urethras of all groups were lined by stratified columnar epithelium. Hemorrhage and mononuclear cells, primarily lymphocytes and macrophages, were not observed in the graft. In the BSM/tissue group, stratified and compressed columnar epithelium three to four layers in thickness lined the luminal surface of the urethra. Newly formed capillaries and bundles of smooth muscle circumferentially surrounded the urethral mucosa, and the muscle layer morphology of the neourethra of the BSM/tissue group was apparently similar to that of controls (Fig. 4E, H). There was no sign of degenerative changes such as calcification or necrosis of the smooth muscle layer. In contrast, the BSM group showed fibrosis-like changes and a simple smooth muscle layer as observed in the stricture group (Fig. 4F, G).
Masson's trichrome staining showed muscle and keratin (red) and collagen (blue) distribution. The primary difference between the BSM/tissue graft and BSM graft groups were the uniformly sized bundles of smooth muscle in the regenerated region. In the BSM/tissue graft group, the composite urethra showed abundant and organized circumferential distribution of bundles of circular smooth muscle similar to the controls (Fig. 4I, L); this finding provided evidence that autologous urethral tissues stimulate rapid cell recovery of the graft. However, the BSM graft showed low muscle distribution, extensive collagen deposition, and keratinized squamous cell epithelium as observed in the stricture group (Fig. 4J, K). On IHC with the pancytokeratin antibody for urothelium staining, the BSM/tissue graft group exhibited uniform pseudostratified columnar and stratified columnar epithelia, as well as stratified squamous cells located near the external urethral orifice as observed in the control group (Fig. 4M, P). The BSM graft group had a thin and irregular epithelia layer, and the thinnest epithelia layer was observed in the stricture group (Fig. 4N, O).
DISCUSSION
The present study is the first to evaluate the application of a combined graft with acellular BSM collagen matrix and autologous urethra tissue for repair of urethral stricture through a nontransected ventral onlay-augmented procedure in an animal model. Traditionally, long segment urethral stricture was managed by substitution urethroplasty using various grafts. For the grafts, buccal-, bladder-, colonic-mucosa, aorta, vein, or skin were commonly used. Although several studies using these grafts showed good results, complications such as graft contracture, necrosis, stricture recurrence, poor elasticity, and urethrocutaneous fistula formation have been also reported (14, 15, 16, 17, 18). Further, for the harvesting of these grafts, additional invasive procedure is inevitable. Recently, metal stent such as Memokath was introducd and used for recurrent urethral stricture, but the success rate was not satisfactory in long sement urethral stricture (19).
To overcome the disadvantages of substitution urethroplasty, onlay procedure have been used. Kim et al. (13) reported satisfactory outcomes with nontransected ventral onlay technique using saphenous vein graft in animal study. In addition, if we use tissue engineering technique for the reconstruction of urethra, additional invasive procedure to harvest graft is not necessary. In order to use grafts as substitutes for the partial segmental replacement of fibrotic urethral tracts, they need to have a suitable length, sufficient elasticity, permit a fluent urine stream, and be absent of hair or mucus formation within the inner layer (20). Tissue engineering techniques have developed human- and animal-derived acellular collagen scaffolds for tissue repair (21, 22, 23). Among these, porcine BSM appears to be a useful biomaterial for tissue repair, owing to its biodegradability, biocompatibility, bioactive molecules, and valuable characteristics such as being thin, flexible, strong enough to suture, and ease of handling (12, 22). In addition, the cellular components are removed through the decellularization process to ensure immunologic safety (22). Several studies on BSM for damaged organ augmentation and vascular replacement have confirmed that BSM promotes regeneration of host tissues (6, 7, 8, 9, 10).
The major difference between the BSM/tissue-grafted urethra and the BSM-grafted urethra was the amount and distribution of the circular bundles of smooth muscle, layers of urothelium, and blood vessels. In addition, retrograde urethrograms revealed relatively proper anatomic urinary width in the BSM/tissue graft group. These differences originate from the embedded urethral tissue. The 3×3-mm2 biopsy tissue from the healthy host urethra enhanced incorporation between host and graft tissue, resulting in rapid tissue regeneration (4). Although there may be concerns about excision of healthy host urethral tissue, these radiologic and histologic study showed the reconstruction of neourethra including the excised portion of normal urethra was properly accomplished. The combined graft was indistinguishable from the native urethral tissue at 12 weeks postoperatively. This combined method did not cause graft contractures, chronic inflammation, or strictures during the experimental period.
BSM/tissue onlay urethroplasty demonstrated evidence of anatomically and histologically normal urethral regeneration on retrograde urethrography, H&E, and IHC. Full-thickness columnar neo-epithelium was observed; the transient urothelium was confirmed by IHC using a pancytokeratin antibody, a useful marker for the identification of urothelium (24), and the grafted portion of the urothelium showed significant pancytokeratin expression. At high magnification, H&E staining revealed that the regenerated urethras showed abundant circular bundles of smooth muscle and some capillaries. Blood vessel formation is a reliable indicator of successful tissue engraftment (25, 26). For the first 3 to 4 days after implantation, grafted tissue obtains oxygen and nutrition from the interstitial fluid; after this period, newly formed blood vessels supply nourishment into the graft. Without full neo-angiogenesis, the graft suffers postoperative ischemia, partial necrosis, and poor function (27).
According to the present results, the BSM/tissue graft showed well-organized incorporation with the recipient tissues. BSM provides a framework for new urethra tissue generated from immigration of the surrounding healthy urethral cells (6), ingrowth of embedded autologous urethra tissue on the graft, and stimulation of the connection between immigrated and embedded cells (4). In contrast, the BSM graft was less effective for urethral regeneration; it showed minimal evidence of regeneration of the urethra, with the graft area lined by squamous keratinized epithelium subjacent to an abundant collagenized fibrous connective tissue backing devoid of any bundles of circular smooth muscle. The excessive deposition of collagen could decrease the flexibility of the tissue (28).
These data suggested that the cells within embedded autologous tissue and BSM can synchronistically act as biological activators for incorporation, promoting ingrowth of surrounding urethral tissue into the scaffold (29). This indicates that the requirement of autologous urethral tissue at the time of implantation is effective for urethral reconstruction. A BSM graft embedded with autologous urethral tissue can be applied for clinical treatment of strictures requiring partially resected urethra replacements.
The limitations of the present study were the small number of rabbits used, the relatively short follow-up period, and the reconstructed urethra was not confirmed functionally such as evaluation of the penile curvature to confirm sufficient elasticity to maintain an erection, uroflowmetry, and anatomic analysis with cystoscopy. Future studies using these methods are needed to obtain a more detailed characterization of the reconstructed urethra.
The present study suggests that BSM/tissue graft used as in urethral onlay urethroplasty is a feasible method for treatment of urethral stricture in an animal model. The BSM/tissue graft demonstrates excellent workability, remains nonimmunogenic, and facilitates the regenerative capacity of the urethra.




 XML Download
XML Download