

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intraventricular hemorrhage (IVH) is the most important cause of mortality and long-term developmental impairment in preterm infants (1). The frequency of definite neurologic sequelae is directly related to the severity of IVH (2). Compared with grade 1/2 IVH, the major neurosensory impairment is almost doubled in severe-grade (grade 3/4) IVH, according to the Papile classification (3). The incidence of severe grade IVH was estimated to be approximately 6 to 16% in the large network cohort of preterm infants with birth weight <1,500 g. Unfortunately, the incidence of severe IVH in extremely preterm infants largely remains unchanged over a decade (4, 5). Every effort has been made to avoid or to minimize the perinatal risk factors for IVH. Studies have proposed the numerous perinatal risk factors of IVH, including low birth weight and gestational age (GA), gender, intrauterine infection, absence of antenatal steroids, mode of delivery, hypoxemia, hypercapnea, pneumothorax, pulmonary hemorrhage, respiratory distress syndrome (RDS), metabolic acidosis, and bicarbonate infusion (6, 7, 8). The pathogenesis of IVH is multifactorial and largely includes the fragility of germinal matrix vasculature, fluctuation in the cerebral blood flow, and disturbances of platelet and coagulation (9).
The association between hypernatremic dehydration and intracranial hemorrhage has been well-described in pediatric patients, including newborn infants (10, 11). However, it is uncertain whether the early change of fluid or serum sodium level can affect the occurrence of severe IVH in preterm infants. Although a few studies have suggested a possible association of IVH with hypernatremia and/or high sodium intake in preterm infants, the cause and effect relationship still remains unclear (12, 13, 14). The purpose of our study is to investigate the association of severe IVH with serum sodium concentration or sodium intake during the early days of extremely low birth weight (ELBW) infants.
MATERIALS AND METHODS
The inclusion criteria of our study were preterm infants with a birth weight <1,000 g who were born and admitted to the neonatal intensive care unit (NICU) at Asan Medical Center from January, 2008 to December, 2012. The exclusion criteria were 1) infants with congenital cardiac/renal anomalies, 2) death prior to the first four days of life or 3) patients whose IVH was identified within the first 24 hr of life by cranial ultrasound performed outside of the routine protocol (see below).
The policy for routine cranial ultrasound in our unit in ELBW infants was to perform it between 24 hr and the first four days of life and thereafter during the first 7 to 10 days of life and by a pediatric neurologist. It was not indicated within 24 hr after birth for initial patient stabilization, although it was sometimes performed at the discretion of attending neonatologists. The grading of IVH was determined according to the Papile classification system (3). For the data analysis, the most severe grade of IVH was chosen within 10 days of life. We categorized the patients into the groups of severe IVH (grade 3/4) and the control (no, grade 1/2 IVH) group.
We recorded the perinatal characteristics including the anthropometric parameters, antenatal steroid, mode of delivery, Apgar scores, RDS, pneumothorax, incidence of hypercapnea (PaCO2≥60 mmHg) and hypocapnea (PaCO2≤30 mmHg), early onset of sepsis (positive blood culture <7 days of life), symptomatic patent ductus arteriosus (PDA) and IVH. Symptomatic PDA was defined by echocardiographic identification of hemodynamically significant left to right ductal shunt with a transductal diameter >1.5 mm and clinical evidence of respiratory or cardiovascular deterioration. Neonatal outcomes included mortality and neonatal morbidities such as PDA ligation, BPD (defined by the oxygen or respiratory support at 36 weeks of corrected age) and retinopathy of prematurity requiring laser therapy.
Data regarding the daily fluid intake and urine output were obtained from our electrical medical records system for each of the first four days of life. Except for the serum electrolyte data on the day of birth (d0), blood gas analyses and serum electrolytes were available in all patients at least once each day during the first four days of life. The maximum and minimum blood PCO2 and serum sodium concentration were also recorded. The daily sodium intake was calculated by adding the sodium amount in parenteral and enteral nutrition, blood products, intravenous fluid, every drug containing sodium salts (Table 1). Specific notations regarding intravenous, sodium-bicarbonate infusions and blood transfusions were also made.
The protocol of fluid therapy and humidification did not change during the study period: for all infants with birth weight <1,000 g, humidification was initiated with 95% humidity from birth to the fourth day of life and was thereafter reduced by 5%-10% each day until humidity of 50% was reached. On the first day of life, the fluid volume was restricted to 70-80 mL/kg/day with 5 or 10% dextrose solution and amino acid solution of 2.0 to 2.5 g/kg/day and was adjusted to maintain a serum sodium concentration within 135-145 mEq/L by monitoring the patient's daily weight, serum sodium, and urine output. Volume intake was generally increased by 10-20 mL/kg/day, reaching 130-140 mL/kg day at 10-14 postnatal days. The contents of electrolytes were modified in the form of an individualized parenteral nutrition solution.
Statistics
A comparison between the severe IVH and the control group was carried out using the Student's t-test or the Mann-Whitney test for determining the continuous variables, and the chi-square test or Fisher's exact test was used for the categorical variables. Among the variables which were significant in univariate logistic regression (cesarean section, RDS, GA, birth weight, Apgar score at one and five minutes, the initial base deficit >5.0 mM/L, any transfusion, and hypercapnea), GA and transfusion were selected by multivariate analysis using the backward elimination method. To determine the associations between severe IVH and the sodium intake and serum sodium concentration, each logistic analysis was performed after adjustment for GA and transfusion. The receiver operating characteristic (ROC) curve analyses were used to determine the cut-off values for the sodium intake and fluid intake. All data analysis was performed using the SPSS version 19.0 (SPSS, INC., Chicago, IL, USA).
RESULTS
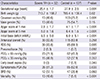
During the study period, a total of 210 ELBW infants was born in the Asan Medical Center NICU. After exclusion of patients with congenital cardiac/renal anomalies (n=9), death prior to four days of life (n=12), and IVH identified within 24 hr after birth (n=20), 169 infants were included in the data analysis. The mean GA and birth weight were 27.0<2.6 weeks and 771.8< 154.1 g. The percentages of any grade IVH and severe IVH were 52.7% (n=89) and 18.9% (n=32), respectively. Compared with the control group, the severe IVH group had a lower gestational age, birth weight, rate of cesarean section and Apgar score at one and five minutes. The base deficit on the initial blood gas analysis and the incidence of RDS, hypercapnea, and symptomatic PDA were also higher in the severe IVH group than in the control group (Table 2).
Except for the day of birth (D0), the daily fluid intake was significantly higher in the severe IVH group than in the control group (Table 3). This was mainly attributable to higher transfusion volume in the severe IVH group versus the control group (Fig. 1). The daily sodium intake was also greater in the severe IVH group than the control group (4.8<3.4 vs. 2.1<1.3, P<0.001). However, besides greater sodium intake from transfusion in the severe IVH group, sodium intake through other fluids also contributed to the significantly higher sodium intake in the severe IVH group (2.3<2.3 vs. 0.5<1.0, P<0.001). The average urine output and percent of weight loss did not differ between the groups. There was also no difference in the incidence of hypernatremia. The maximum and minimum sodium concentration and the degree of sodium fluctuation did not differ between the two groups (Table 3).
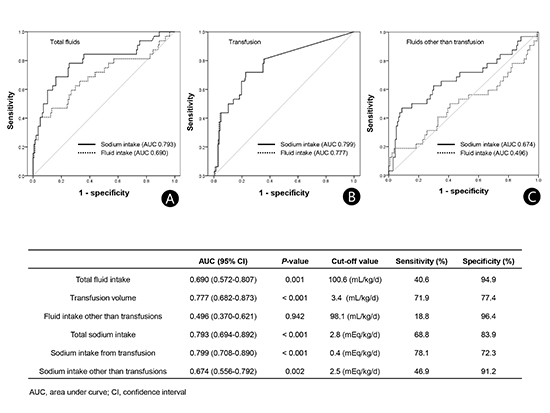
The ROC curves regarding the association of severe IVH with sodium and fluid intake from total fluids, transfusion and fluids other than transfusion were plotted (Fig. 2). Related to the fluid balance and sodium intake, the risk for severe IVH was strongly associated with total fluid and sodium intake during the initial four days of life. With respect to the fluids other than transfusion, severe IVH can be discriminated only by sodium intake and the mean cut-off value of the sodium intake was 2.8 mEq/kg/day as the point maximizing the sum of the sensitivity and specificity.
The odds ratio of severe IVH was plotted with the mean daily fluid and sodium intake after adjustment for GA and transfusion (Fig. 3). The intake was stratified by the interval of arbitrary cut-off value of 5 mL/kg/day (for fluid intake) and 0.5 mEq/kg/day (for sodium intake), respectively. During the first four days of life, there was an increase in the risk of severe IVH with total sodium intake >3.0 mEq/kg/day or sodium intake from fluids other than transfusions >2.5 mEq/kg/day. However, no clear relationship was demonstrated between the risk of severe IVH and fluid intake other than transfusion.
DISCUSSION
In our study, the amount of sodium and fluid intake within the first four days of life, and particularly, sodium intake from fluids other than transfusions were significantly associated with severe IVH in ELBW infants. Few comparative studies have been conducted which were focused on the association between sodium intake and IVH in preterm infants. In a small prospective study in 17 very low birth weight (VLBW) infants, the incidence of IVH did not differ between the sodium-restricted group and the sodium-maintenance group, with a mean daily intake of 0.85 mEq/kg/d and 4.33 mEq/kg/d, respectively, although the dose of "inadvertent" sodium intake was not specified (15). A recent observational study by Barnette et al. (12) demonstrated a clear dose-response relationship between the early sodium intake and IVH of ≥grade 2 or more in the VLBW infants after controlling GA, the most important determinant of developing IVH. Using a similar study design to that study, we again demonstrated the increased odds ratio of severe IVH associated with an average sodium intake >2.5 mEq/kg/day from fluids other than transfusions after controlling for both GA and blood transfusions. The threshold of mean sodium intake in our patient cohort of ELBW infants was seems to be lower than the value in Barnette's study (>4.5 mEq/kg) (12). However, we have not determined if the ELBW infants are more vulnerable to IVH at the same level of sodium intake than VLBW infants.
Besides the sodium intake through transfusions, the reason why the patients in the severe IVH group received more sodium than the control group remains unclear. The higher sodium intakeparticularly during the first 4 days of life in the severe IVH group simply might reflect the higher basal requirement of saline-based fluids for maintaining catheter patency for patient monitoring in the severe IVH group as they are at greater risk of hemodynamic instability than the control group. Another explanation is more crystalloid infusion to treat low blood pressure or low urine output in the severe IVH group than in the control group. However, the mean fluid intake other than transfusions did not differ between the groups. This is in accordance with a recent Cochrane analysis (16), where there was no difference in the incidence of all grade IVH between the volume restriction groups and the liberal fluid intake groups. The possibility of caregiver's preference to administer more amount of sodium through the parenteral nutrition to strictly control the serum sodium concentration in the severe IVH group that demonstrated more fluctuations in the serum sodium levels cannot be completely excluded. However, this cannot be verified in this retrospective study.
We were unable to identify a significant correlation between the serum sodium concentration and the severe IVH in our study. The causality of early hypernatremia in the development of IVH in preterm infants has been conflicting in the published studies. Although a few studies published during the pre-surfactant era raised concerns regarding the risk of liberal and excessive sodium bicarbonate administration in the development of IVH (17, 18), the pathogenesis of IVH using this strategy may be attributed to altered cerebral blood flow caused by hypercarbia and/or rapid volume expansion rather than by hyperosmolarity per se (19, 20, 21). Lupton et al. (22) revealed that a high serum sodium concentration during the initial four days of life, when defined by serum sodium >145 mM/L or >152 mM/L, was not associated with an increased risk of IVH in VLBW infants. A few case reports regarding extremely preterm infants who showed normal development after exposure to extreme hypernatremia, also support this finding (23, 24). Meanwhile, a case-control study by Lim et al. (14) demonstrated the difference in the highest serum sodium level and the difference in the serum sodium between the IVH and the control groups in the GA and the birth-weight matched cohort. However, they did not address the incidence or risk of hypernatremia defined by a specific threshold of serum sodium. Another large study by Perrott et al. (25) also demonstrated the significant association of hypernatremia (>155 mmol/L) with major neurodevelopmental disability in the preterm infants with <30 weeks of GA, although the association with IVH was not directly documented. As with the issue of sodium intake, the causal relationship of the serum sodium level and severe IVH cannot be elucidated by retrospective studies, including ours.
Our study is clearly limited by its retrospective nature. Despite the control of many confounders, the causality of high sodium intake and IVH can only be determined by large, prospective, comparative trials. The timing of head ultrasound is another limitation for the data analyses, although we excluded those patients whose IVH was identified within 24 hr after birth. Exclusion of the patients who died early and were thus free of insufficient data for sodium and fluid might have affected our study outcome. The severity of IVH was only graded using the Papile classification. The type of intracranial hemorrhage following hypernatremic dehydration differs from the type of IVH or periventricular hemorrhagic infarct in preterm infants in that it demonstrates diffuse linear cerebral lesions, particularly at the gray-white matter junction and in multiple intra- and extra-parenchymal hemorrhage which eventually leads to diffuse encephalomalacia (26, 27, 28).
In conclusion, along with the previous studies favoring early sodium restriction in the prevention of neonatal morbidities in preterm infants (12, 13, 15), the impact of the sodium restrictive strategy on the development of IVH in ELBW infants should be determined by a large, randomized controlled trials which allows a wide range of serum sodium concentrations.




 XML Download
XML Download