

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Iodinated contrast media (ICM) are widely used for enhancing radiographic contrast and the diagnosis, treatment and monitoring of various diseases. A previous report revealed that the frequency of ICM administration in clinical practice was approximately above 75 million times in a year (1). In addition, the use of ICM is growing rapidly worldwide. Adverse reactions after administration of ICM are not rare. Toxic reactions such as nephrotoxicity (2) or neurotoxicity (3) as well as unpredictable hypersensitivity reactions to ICM are well known.
Hypersensitivity reactions to ICM are one of the most common causes of serious adverse drug reactions including anaphylaxis in hospitals (4, 5). Hypersensitivity reactions to ICM are classified according to the time interval between ICM exposure and the first appearance of symptoms as immediate reactions occurring within 1 hr after exposure or non-immediate ones, commonly cutaneous manifestations, occurring 1 hr to several days (6).
The prevalence of ICM hypersensitivity is dependent on types of ICM. With replacing ionic ICM to nonionic ones, the frequency of adverse reactions to ICM has been gradually reduced. Immediate reactions have been reported up to 12.7% of patient receiving ionic ICM, whereas those to non-ionic ICM occurred in 0.02%-3.1% of ICM administration (6). The frequency of non-immediate reactions varies from 0.5% to 23.0% (7). Anaphylaxis, urticaria, angioedema, rhinitis, dyspnea, and hypotension are common clinical phenotypes of immediate hypersensitivity, while maculopapular exanthemes are the major manifestation of non-immediate reactions (6).
The mechanisms of immediate hypersensitivity have been considered as nonallergic reactions. For examples, 1) direct secretary effects on mast cells or basophil possibly related to the local changes in osmolality, 2) activation of the complement system, and 3) direct bradykinin formation (8, 9, 10). However, there is growing evidence that the mechanism of immediate hypersensitivity to ICM may be IgE mediated, and that of delayed skin rashes is T cell mediated (10, 11, 12, 13). Increased levels of histamine and tryptase were demonstrated in plasma from patients with immediate hypersensitivity reactions to ICM (14). In addition, serum specific IgE to ionic ICM was detected in a small group of patients with severe immediate reactions after exposure to ICM (15). The histopathologic findings of skin eruptions to ICM are comparable with other T-cell mediated reactions as like a dermal lymphocyte rich infiltrate accompanied by intradermal spongiosis (13). An European multicenter study reported that at least 50% of immediate reactors and up to 47% of non-immediate reactors were positive on skin tests (16).
Although it was proved that intradermal skin test (IDT)s with ICM for the purpose of prescreening is not useful to predict adverse reactions (17), the positive rate of skin test results to the culprit ICM was 47.8% in patients with anaphylaxis to ICM in Korea (5). Recently, patch tests and delayed interpretation of IDT are suggested to evaluate non-immediate hypersensitivity reactions to ICM (18). However, there is a few and limited data to determine the clinical utility of immunologic evaluation of ICM in Korea. This study was aimed to investigate the potential utility of ICM skin testing including skin prick, IDT (early and delayed reading), and patch tests in patients with ICM hypersensitivity and to identify safe substitutes for the patients who are supposed to get repetitive ICM-based evaluation and treatment.
MATERIALS AND METHODS
Subject
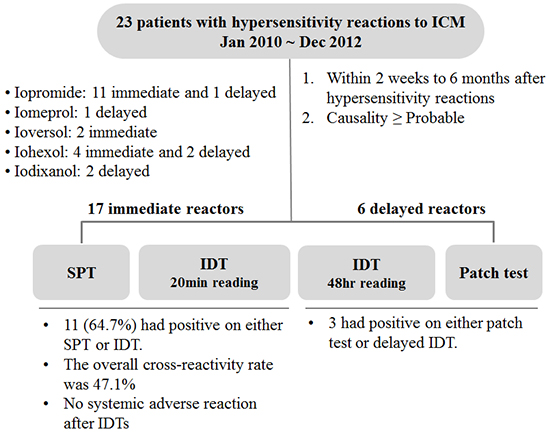
Total 23 patients (17 immediate and 6 delayed hypersensitivity reactions) with probable or certain causality based on the WHO-UMC assessment were enrolled from 3 Pharmacovigilance centers in Korea including Ajou University hospital, Chonnam National University hospital, Hallym University hospital, between January 2010 and December 2012 (Fig. 1). Patients with severe ICM reactions like toxic epidermal necrolysis, Stevens-Johnson syndrome, acute generalized exanthematous pustulosis were excluded in this study. As a control group, age and gender adjusted 10 non-atopic healthy subjects were recruited from Ajou University hospital. Demographics, history of previous ICM induced adverse reactions, latent period, time interval between hypersensitivity reactions and testing, culprit ICM, medications, co-morbidities including allergic disease, malignancy, diabetes, and hypertension were obtained. Patients who had been taking medications such as steroid and antihistamines that may have affected skin test results, had ongoing hypersensitivity reactions or severe cardiovascular diseases were excluded.
Skin testing with ICM
Hypersensitivity reactions were defined according to the time interval between ICM administration and symptom onset as immediate (<1 hr) and non-immediate (1 hr to 1 week). ICM skin testing was performed for the subjects within 2 weeks to 6 months after hypersensitivity reactions. Skin prick (SPT), IDT and patch tests were carried out with a series of 6 commonly used ICM; iopromide, iohexol, ioversol, iomeprol, iopamidol and iodixanol (Fig. 1).
SPTs and IDTs were conducted on the right and left forearm volar area, respectively. SPT and patch test were performed by applying undiluted contrast media, whereas intradermal test was done by applying 100-fold diluted contrast media for the patients with anaphylaxis and then went up to 10-fold diluted and undiluted ones. SPT was read after 20 min; the result considered positive when the diameter of wheal increased by at least 3 mm surrounded by erythema. Delayed intradermal test positivity was determined when erythematous induration was observed on day 2 or day 3. Histamine (0.01%) and saline were used as positive and negative controls, respectively. Patch test was conducted on the patients' back. ICM soaked on filter paper in 12 mm aluminum chamber, fixed with adhesive tape on the back for 2 days. Skin readings were performed 15 min after removal of the strips on day 2 and day 4 according to the clinical scoring criteria recommended by the International Contact Dermatitis Research Group (19).
Statistical analysis
SPSS version 19 (SPSS Inc., Chicago, IL, USA) was used for the analysis. All values were expressed as means±standard deviation. Fisher's exact test was used for categorical data. The t-test was used for continuous data.
Ethics statement
The study was approved by the institutional review board of the study hospitals (AJIRB-MED-SUR-09-305 and 2014-0333 in Ajou University hospital, 2010-07-125 in Chonnam National University hospital and 2011-I023 in Hallym University Sacred Heart hospital). All patients provided informed consents.
RESULTS
Baseline characteristics of subjects
A total 23 subjects with a history of ICM-induced hypersensitivity reactions within recent 6 months before the enrollment at least one ICM were evaluated. Mean age of the subjects was 50.1±16.4 yr and 43.5% were male patients (Table 1). Twelve (52.2%) of them had been exposed to ICM in the past. Three (2 urticaria and 1 anaphylaxis) of them had hypersensitivity reactions after the previous exposure. Six subjects (26%) had malignancies or hypertension, respectively. Seven subjects (30.4%) were atopic, 4 (17.4%) had a diagnosis of drug allergy. Anaphylaxis was occurred in 10 (58.8%) of the immediate hypersensitivity group.
Iopromide (52.2%) was the most frequently reported ICM, followed by iohexol (26.1%), ioversol (8.7%), iodixanol (8.7%), and iomeprol (4.3%). The examinations carried out were a CT scan in 22 (95.7%) and coronary angiography in 1 (4.3%). The mean latent period from ICM administration to first appearance of symptoms was 11.5 min and 19.3 hr in patients with immediate and non-immediate hypersensitivity group, respectively. The mean time interval between hypersensitivity reactions and skin testing in patients with immediate hypersensitivity group was 119.9 days, whereas in patients with non-immediate hypersensitivity group was 32.3 days.
Skin test results
Of 10 patients with anaphylaxis, 3 (30.0%) and 6 (60.0%) were positive respectively on SPTs and IDTs with the culprit ICM. Three of 6 patients with urticaria showed positive IDTs (Table 2). Of the 14 cases with immediate reactions showing a negative SPT, 9 had a positive response to IDT. Of the 10 cases with a positive IDT, 3 had a positive response on a 10-fold diluted medium, whereas another 7 had a positive reaction only on undiluted media. In total, 11 (64.7%) had positive on either SPT or IDT. No systemic adverse reaction after IDTs even with undiluted media for the patients with a history of anaphylaxis was observed in the present study. One of 6 patients with delayed eruptions had positive response to both patch test and delayed IDT. Each of other two patients showed positive result on either patch test or delayed IDT. Iopromide (6 anaphylaxis and 5 urticaria) and iohexol (2 anaphylaxis and 2 urticaria) are more commonly associated with immediate hypersensitivity. Iodixanol and iohexol are more frequently related to delayed hypersensitivity. None had a positive reaction with skin testing with ICM in the control group. In addition, the skin test positivity was compared by 2 months of the time interval between hypersensitivity reactions and skin testing. Seven (77.8%) of 9 patients taken skin testing between 2 months and 6 months after occurring immediate hypersensitivity reactions had a positive response to the culprit, whereas 50% of the patients whose skin testing was performed within 2 months from the hypersensitivity reactions showed positive results on the skin test.
Cross-reactivity
The overall cross-reactivity rate of immediate reactions was 47.1% and that of delayed reactions was 33.3%. Of the 11 cases with positive IDT, 3 were positive to one ICM, 3 to three ICM, and 5 to all the tested ICM. Among 6 patients with delayed reactions, 1 case was positive to all the tested ICM in delayed reading of IDT. The crossreactivity of ICM skin test in patients with immediate hypersensitivity to iopromide (Fig. 2) as follows; 57.1% (n=4/7) in iohexol, 50.0% (3/6) in iopamidol, 42.9% (3/7) in ioversol, 33.3% (2/6) in iodixanol. One patient who had taken IDT with iomeprol showed positive result, too.
Additional ICM after the study period
Among 5 patients (3 anaphylaxis, 1 urticaria and 1 delayed rash) taken subsequent radiologic examinations after completing this study, 3 patients (2 patients with iopromide-induced immediate reactions and one with iodixanol-induced delayed reaction) administered safe alternatives, such as iopamidol or iohexol, in accordance with the skin testing results, had no adverse reaction. However, in spite of premedication with oral steroid and antihistamines, anaphylaxis was developed again in the other 2 patients who received the positive ICM on the previous skin test (Table 3).
DISCUSSION
In the present study, we confirmed 64.7% of the sensitivity of skin testing with culprit ICM for 17 patients with immediate hypersensitivity reactions after recent exposure to ICM. In addition, even in very small number of subjects, 50% of patients with delayed hypersensitivity to ICM showed positive reactions on patch test and/or delayed intradermal test. A recent study using the database of adverse event (AE)s reports from 15 Regional Pharmacovigilance Centers in Korea reported that the most often AEs of ICM were allergic reactions, such as urticaria, pruritus, angioedema, hypotension, anaphylaxis, and dyspnea, and gastrointestinal and urinary system disorders (20). The most commonly implicated ICM were iopromide and iohexol. In addition, these 2 ICM were frequently associated with anaphylactic reactions or other allergic reactions, whereas urinary system disorders were significantly higher for iodixanol (20). We also found that the most common culprit ICM in patients with immediate hypersensitivity was iopromide in the present study.
Immediate and delayed hypersensitivity reactions to ICM, whether those are mediated by immunologic or non-immunologic mechanisms, are unpredictable AEs, but occasionally result in serious outcomes. To prevent ICM-induced AEs, pretesting with an intravenous injection of ICM had been conducted in the 1970s. However, this approach was abandoned due to a lack of evidence. Sometimes severe cardiovascular reactions were developed after the pretest itself (21). In a previous Korean report, the clinical utility of prescreening skin test right before ICM administration was not demonstrated (17). They reported that none showed a positive response to prescreening skin tests with the suspected ICM among the 61 cases with previous immediate hypersensitivity reactions to ICM, while 52 of the 1,046 patients with a negative response experienced immediate reactions after exposure to ICM. It has been common practice to take premedication with corticosteroids and/or antihistamines for patients with a history of severe adverse reactions to ICM (21). However, severe anaphylactic reactions to ICM may be recurred in patients who had experienced previous ICM-induced reactions in spite of premedication. Kim et al. reported that overall recurrence rate after premedication with corticosteroid and H1 antihistamines and/or H2 blockers was 16.7% in 30 prior reactors (22). Therefore, needs for the establishment of clinically useful tests in order to confirm the cause and find safe alternative ICM for the patients with ICM hypersensitivity are still unsatisfied.
Recently, the understanding of the pathophysiology of ICM-induced hypersensitivity reactions has been expanded. But, the mechanism underlying adverse reactions to ICM is complex and not yet completely elucidated. Although some patients can have adverse reactions on their first exposure to ICM, a previous hypersensitivity reaction is well known as an important risk factor for new reactions on repeated exposure. It also supports that immune-mediated hypersensitivity may be involved in both immediate and delayed reactions to ICM. Skin tests have been performed in the diagnosis of hypersensitivity reactions to ICM for a long time (13, 16, 21), as like those are applied to confirm a drug allergy, such as beta-lactam allergy (23). The positivity rate of the tests varied depending on types of ICM, time interval between the occurrence of reactions and the evaluation performed, and the severity of reactions. A recent European multicenter study reported that 96.3% of the specificity and 50% of the sensitivity were obtained when IDT with ICM was conducted within the optimal time period 2-6 months after the reaction and for whom had the knowledge on the culprit ICM (16). However, the studies conducted regardless of the precise information of the culprit ICM for each patients revealed the lower frequency of skin tests positivity (16, 24). They found positive IDTs just in 28% of the 32 patients (24) and 24.6% of the 122 patients (16) because 60% and 48% of their subjects had no idea on the culprit ICM in the two studies, respectively. As similar with the present study, a recent French study performed on the 26 patients having the precise knowledge of the culprit showed that the sensitivity of IDTs with ICM was 73.1% (25).
In addition, the positivity rate of immediate IDT with ICM increased in patients with severe hypersensitivity reaction compared with mild reactors (5, 17, 25). It varies from 12.9% or 56% in grade I reactions to 57.1% or 100% in grade III or IV reactions in a previous studies (17, 25). Even in the cases with anaphylaxis to ICM, it was quite different between patients with anaphylactic shock (81.8%) and normotensive anaphylaxis (33.3%) (5). The optimal ICM concentration for use in IDT is not established. Some investigators have tried to use undiluted ICM in IDT if the patients had a negative response to a 10-fold diluted one (25, 26). Dewachter et al. reported that 36.8% of 19 patients with positive IDTs were confirmed with undiluted ICM (25). In the present study, we enrolled patients who had experienced hypersensitivity reactions to ICM within 6 months and whose culprit ICM of previous reactions were already identified. The positive IDTs for the 11 patients with immediate reactions were obtained with the ICM diluted at 1:100 in 1 case, 1:10 in 2 cases and with undiluted ICM in 8 cases. As like previous studies applied undiluted ICM (25, 26), no systemic adverse reaction was observed in the present study.
Through the results in the 5 patients who have taken subsequent radiological examinations after the completion of this study, we supported that skin testing can help to select safe alternatives and to avoid potential crossreactive ICM for the patients with hypersensitivity to ICM. In particular, as in our study, most patients with ICM hypersensitivity are supposed to take ICM-based evaluation or treatment repeatedly because they have malignancies or cardiovascular diseases for which regular monitoring and intervention is usually required. Therefore, the confirmation of the causative ICM and crossreactants to be avoided is necessary for the patients with severe ICM hypersensitivity including anaphylaxis when repetitive exposure to ICM is expected. Although this study shows 64.7% (11/17) and 50% (3/6) of the sensitivities of corresponding skin tests with culprit ICM for immediate and delayed hypersensitivity reactions respectively, limited number of study subjects particularly in the delayed hypersensitivity group does not allow us to make a concrete conclusion within this study. But, these data support the potential utility of IDT with commonly used ICM for patients with previous immediate ICM hypersensitivity to suggest possible crossreactivity among other ICM.
In conclusion, skin testing, particularly, IDT with undiluted ICM performing within 6 months after prior hypersensitivity reactions, can be useful at least for patients with ICM-induced anaphylaxis to confirm the diagnosis and to select safe alternative ICM. However, further investigation is necessary to determine the predictive values of skin tests with ICM and to understand immunological mechanisms of ICM hypersensitivity reactions.





 XML Download
XML Download