

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Potocki-Shaffer syndrome (PSS, OMIM #601224) is a rare contiguous gene deletion syndrome caused by heterozygous deletions within chromosome 11p11.2p12 (1, 2). Characteristic clinical features include craniofacial anomalies, multiple exostoses, bilateral parietal foramina, abnormalities of genitourinary system, hypotonia, developmental delay, and intellectual disability (1, 2, 3). Fewer than 40 cases have been reported in the literature (4), and there was no reported Korean patient.
Analyses of clinical and cytogenetic data from patients with various sizes of deletions in the 11p11.2p12 have demonstrated that the two genes within the interval, EXT2 and ALX4, are responsible to the phenotypes (5, 6, 7). EXT2 and ALX4 have been implicated in formation of exostoses and enlarged parietal foramina, respectively (1, 3, 4, 5). However, haploinsufficiency of these two genes can explain only skeletal abnormalities. Recently, PHA21F was suggested as a responsible gene of craniofacial abnormality and intellectual disability phenotype of patients with PSS (8). In addition, Montgomery et al. (4) reported a patient with developmental delay and hypotonia resulting from a 137-kb small deletion in PSS interval on 11p11.2 including PHA21F.
Through a chromosomal microarray approach combined with clinical manifestations and radiographic findings, we present a first Korean patient with PSS.
CASE DESCRIPTION
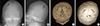
An 8-yr-old boy was referred to the department of medical genetics on February 25, 2014 for severe global developmental delay and multiple exostosis detected in radiologic check up. The patient was born to healthy nonconsanguineous Korean parents after 40 weeks gestation with birth weight of 2,400 g (<3 percentile). He had no perinatal problem. His developmental delay was noted when he was 3 month of age because of incomplete eye contact and head control. Physical examination revealed hypotonia, ptosis, nystagmus and microcephaly with craniosynostosis. Given the child's developmental delay and craniofacial dysmorphism, peripheral blood chromosome analaysis was done and the karyotype was 46,XY. At the age of 8 month, He had expansion cranioplasty for craniosynostosis. His developmental delay became profound. At 45 months, he could neither sit alone nor saying a meaningful word. Surgery for strabismus was performed. When he was at age 5 yr, he received Korean-Wechsler Preschool and Primary Scale of Intelligence (K-WPPSI) testing. His full-scale Intelligence Quotient (IQ) composited score of less than 30, considered severe intellectual disability. By Social Maturity Scale (SMS), his social quotient (SQ) was 17.8 and social age was measured as 0.91 yr. At 6 yr, protrusions of the right wrist and knee were noted. Skeletal survey revealed multiple exostoses throughout the long bones (Fig. 1). However, the underlying cause of the multiple exostoses was not found at that time. At 8 yr, the progression of multiple exostoses was noted and the patient had thoroughly re-evaluated the clinical data and radiographs taken from the age of 4 months. Initial skull radiographs and 3D reconstructed image showed premature craniosynostosis of the coronal suture and large biparietal foramina (Fig. 2A). Brain MRI revealed cortical atrophy with mild ventriculomegaly. Because of premature craniosynostosis, he received expansion cranioplasty of the coronal suture at age 6 months. Follow-up skull examination at age 8 yr showed persistent biparietal foramina but much decreased in size (Fig. 2B). Physical examination at age 6 yr, his growth was severely retarded, height was 96 cm (<3 percentile), weight was 15.7 kg (<3 percentile), and head circumference was 45 cm (<3 percentile). Facial features showed sparse eyebrows, nystagmus, prominent nasal bridge, hypoplastic nare, down turned mouth and high arched palate. The patient was hypotonic. He could not sit or walk alone. Review of the chart, diagnosis was craniosynostosis and mental retardation only.
Based upon the retrospective review of the clinical chart and radiographs, PSS was firstly suggested and chromosomal microarray analysis using CytoScan™ 750K (Affymetrix, USA) was performed. The array is characterized with>750,436 CNV markers including 200,436 genotype-able SNP probes and 550,000 non-polymorphism probes. With informed consent, genomic DNA samples were extracted with Qiamp DNA Blood mini kit (Qiagen, USA) from peripheral blood. All data was visualized and analyzed with Chromosome Analysis Suite (ChAS) software Package (Affymetrix, USA) using genome build Hg 19. The chromosomal microarray revealed an 8.6 Mb deletion at 11p11.2p12 [arr 11p12p11.2 (Chr11:39,204,770-47,791,278)×1] and confirmed the molecular diagnosis of PSS. This deletion resulted in haploinsufficiency for all three genes, included EXT2, ALX4, and PHA21F (Fig. 3). After diagnosis of PSS, the patient continued rehabilitation therapy for profound developmental delay. The progression of multiple exostosis or developing pain have being monitored by radiologic exam every 6 month for need of surgical intervention.
DISCUSSION
As PSS is a contiguous gene deletion syndrome, the phenotypical spectrum is highly variable depending on the deletion size and location. With advancing genomic diagnostic tools such as microarrays, microdeletion syndromes which were hard to identify by conventional cytogenetic methods, are having been improved its diagnostic efficiency. Chromosomal microarray applied in this case would be useful to further analysis of genotype-phenotype correlation by identifying the breaking points and deletion sizes. The typical PSS phenotype requires deletion of at least 2.1 Mb, spanning form D11S1393 to D11S1319, including EXT1 and ALX4 (4, 7). Our PSS patient revealed a large deletion with 8.6 Mb (Chr11:39,204,770-47,791,278) extending to 11p12, which included all three responsible genes, EXT1, ALX4, and PHF21A. As our patient had relatively large size of deletion comparing to the previously reported range of deletion size (4.48 to 8.64 Mb) (2), he might be presented with typical skeletal abnormalities, motor developmental delay, and severe intellectual disability.
Multiple exostoses is a condition characterized by multiple cartilage-capped boney protuberances, arising from the metaphyses of long bones (9). The majority of patients have mutation of EXT1 or EXT2. Patients with PSS have multiple exosotoses resulting from deletion of EXT2. Together with the exostosin-1 (EXT1), the exostosin-2 (EXT2) is known to be involved heparan sulfate elongation in a heteroligomeric complex in the Golgi apparatus of most human cells (10, 11, 12). Heparan sulfate is one of the sugar chain that can be added to specific proteins headed for the cell surface and extracellular matrix. In multiple exostoses, in which EXT expression is decreased by mutation or deletion, the heparan sulfate proteoglycans seem to accumulate in the cytoplasm of the cell, instead of being transported to be expressed at the cell surface, which resulted in expression of exostosis (13).
Parietal foramina are the resulting from delayed or incomplete ossification of the parietal bones of the skull. Parietal foramina can occur as either an isolated autosomal dominant trait or as part of a syndrome (14). As ALX4 located in 11p11.2, deletion in this interval specifically were shown to be expressed in bones and involved in skull development, and thus haploinsufficiency of ALX4 resulted in biparietal formina in patients with PSS (14).
Recently, Kim et al. (8) reported that disruption of PHF21A by translocations in the PSS region is associated with intellectual disability adds to the growing list of ID-associated genes that emphasize the critical role of transcriptional regulation and chromatin remodeling in normal brain development and cognitive function. Moreover, Montgomery et al. (4) strengthened the role of PHF21A in intellectual disability in PSS. Resulting from the large size of deletion including these three genes, our patients might have severe mental retardation and typical skeletal findings (multiple exostoses and bilateral parietal foramina).
In terms of clinical and radiologic findings, we could not diagnose him having PSS till his progressive multiple exostoses were noted when he was the age 8 yr. Among many etiologies of multiple exostoses including EXT mutations, PSS would be a one of the rare cause presenting exostoses. Therefore, a patient with multiple exostoses accompanying syndormic features including craniofacial abnormalities and mental retardation, the diagnosis of PSS should be considered and should be assessed by chromosomal microarray.
Because PSS is an incurable genetic disease, treatment is conservative. For the health maintenance, multidisciplinary approach and continuous monitoring of growth and development is essential. Early childhood intervention of developmental delay at the time of diagnosis is needed. A full skeletal survey is recommended at the time of diagnosis or by age 3 yr (2). Surgical intervention should be considered in case of pain or deformity of bones. As the prognosis of patient depends on the severity of developmental delay and neurologic deficit, the follow up of clinical manifestation is warranted in our patient.


 XML Download
XML Download