

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Vitamins are micronutrients that are essential to the maintenance of organ functions. Vitamin deficiency causes various complications such as classic vitamin deficiency syndromes like scurvy, and associations of vitamin deficiencies and several clinical conditions like cardiovascular disease, immune dysfunction and infectious disease have been reported (12345). One of the most serious health problems of the homeless is their generally poor nutritional status. As alcohol tends to be the major source of calories, for those who abuse it, vitamin and other micronutrient deficiencies are all-too-common ailments (6789).
Few studies have focused on the vitamin status of homeless patients who have visited to an emergency department (ED). And perhaps counterintuitively, several reports have shown that vitamin deficiency, especially of vitamin B complex, is not common among patients visiting an ED after excessive alcohol ingestion (1011). In the present investigation, we evaluated the actual vitamin statuses of alcoholic homeless patients who visited our ED. Our hypothesis was that vitamin deficiency is common in homeless patients and that diminished vitamin levels are correlated with higher admission rates.
MATERIALS AND METHODS
Study design
This study was a retrospective chart review conducted at a single academic teaching hospital with 53,000 annual ED visits. Electronic medical-record data covering the period from January to November 2013 were reviewed. The collected data included demographics such as age and sex as well as information on underlying diseases, laboratory tests, diagnoses and ED dispositions. Patients whose blood levels of vitamin B1, B12, B6, and C were checked and treated in the homeless observation area of the ED were enrolled. Data collection and analysis were conducted from March to July 2014.
Study subjects
All of the patients were treated by trained triage nurses according to the emergency severity index (ESI) (12). All of the ESI level 1 or 2 patients, including level 1 and 2 homeless patients, were moved either to the resuscitation area or the acute care and monitoring area, as individual circumstances dictated. Meanwhile, all of the homeless patients excepting those of level 1 or 2 were moved to a special observation area allocated for the homeless. The initial evaluation and stabilization were conducted there. The attending emergency physician ordered vitamin levels if patients were alcohol-intoxicated and needed intravenous fluid hydration, or basic laboratory tests. These were the patients deemed eligible for analysis. All samples were drawn prior to administration of intravenous fluids or medications. After the initial evaluation and stabilization, individual dispositions were determined based on clinical conditions. Patients were permitted to stay several days in the ED if they desired, providing that they did not have any specific diseases.
Measurement
Vitamin B1, B6, and C levels were assessed by subjecting blood samples to high performance liquid chromatography (HPLC) (Perkin-Elmer Series 200, PerkinElmer, Inc., Waltham, Massachusetts, US). The vitamin B12 levels were determined by electrochemiluminescence immunoassay (Roche E170, Roche Diagnostics, Basel, Switzerland). Because the maximal vitamin B12 measurable limit at our center is 1,800 pg/mL, values over 1,800 pg/mL were regarded as 1,800 pg/mL for the purposes of the analysis.
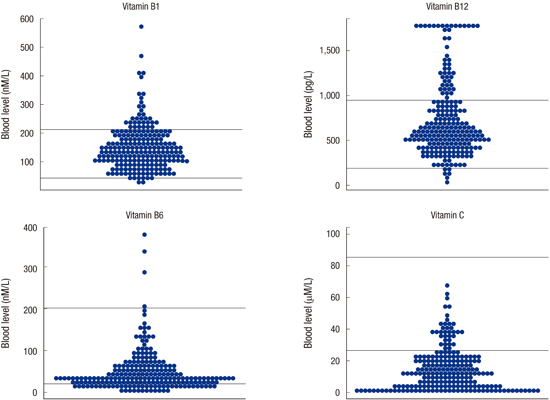
In our hospital laboratory, Vitamin B1 levels of 59 to 213 nM/L, B12 levels of 200 to 950 ng/L, B6 levels of 20 to 202 nM/L, and C levels of 26.1 to 84.6 nM/L were considered normal.
Statistical analysis
The Shapiro-Wilk test was used to evaluate the normality of the continuous variables. Because none of the continuous variables were normally distributed, the Wilcoxon-Mann-Whitney test was used. Data are presented as median and interquartile range. For the categorical variables, chi square test or Fisher exact test was used as appropriate. All of the analyses were performed with R, version 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria). A P value of 0.05 or less was considered to indicate statistical significance.
RESULTS
Vitamin levels were examined in 217 patients during the study period. The patients' mean age was 51 yr, and 8.8% had some form of infection. One hundred and seventy-three patients (79.7%) were discharged, 25 (11.5%) were admitted, 5 (2.3%) were transferred to a lower-tier hospital, 13 (6%) disappeared, and one (1%) died (Table 1).
With regard to vitamin C, 84.3% of the patients had blood levels below the reference range. As for vitamins B1, B12, and B6, 2.3%, 2.3%, and 23.5% of patients, respectively, had blood levels below the reference range. No patient showed a vitamin C level above the reference range (Tables 1 and 2, Fig. 1).
The vitamin C levels of the admitted patients (including those transferred) were all lower than those of the discharged and lost patients (13.25 [3.9-22.2] µM/L vs. 7.7 [1.8-11.1] µM/L, P=0.003). None of the other vitamin levels were significantly differed between the admitted and discharged patients (Fig. 2). Information about smoking status was available for 112 (51.6%) patients, 90 (80.4%) were smokers and 22 (19.6%) were non-smokers. The differences in the vitamin B1, B12, B6, and C levels between the smokers and nonsmokers were not significant (Table 3).
DISCUSSION
Micronutrient deficiency is common in cases of chronic disease. The homeless are exposed to many chronic ailments and infirmities, and their access to medical services is limited. A common nutrition source for homeless people, moreover, is alcohol, and indeed, in cases where alcohol is seriously abused, many kinds of vitamin deficiencies are to be expected (6891113).
Thiamine, the lack of which causes Wernicke's encephalopathy, is believed to be insufficient in alcoholics, as are many other vitamins. However, Li et al. (10) reported no cases of thiamin or folate deficiency among 75 acutely alcohol-intoxicated patients in an ED. They concluded that routine supplemental intravenous vitamin complex doses are not required for acute-alcohol-intoxicated patients.
Malmauret et al. (9) evaluated the vitamin levels of homeless individuals in four CHUSI units (emergency homeless shelters). High alcohol consumption and vitamin C deficiency both were very common (95%). The rates of vitamin A, B1, B6, B12, and E deficiency were 43.6, 5.6, 5.6, 14.1, and 19.7%, respectively.
In our study, four vitamin levels were evaluated. Vitamin C deficiencies were very common (84.3%), and no patient showed an excessive blood level. Vitamin B1 or B12 deficiency, by contrast, was not common; in fact, 17.5% of the vitamin B1 and 23% of the vitamin B12 levels were higher than the respective reference ranges. These findings, which can be summarized as a low incidence of vitamin B complex deficiency and a high incidence of vitamin C deficiency, respectively, match those of previous studies (910). Also in our study, the vitamin B1, B12, and B6 overexposure rate were 17.5%, 1.8%, and 23%, respectively, markedly lower than those of the French study (in which vitamins B1, B12, and B6 overexposure were found in 35.2%, 50.7%, and 42.2% of patients, respectively) (Table 2, Fig. 1) (9). Our study population was comprised of homeless patients of a tertiary hospital ED and some of whom had acute medical conditions such as acute infection (8.8%), acute appendicitis (0.5%), pancreatitis (1.4%) and trauma (20.7%) (Table 1). These acute conditions are risk factors for exhaustion of the human vitamin reservoir (141516).
Among the four vitamins at issue, only the vitamin C levels were related to the admission rate. They were lower in the admitted patients, and the difference was statistically significant. Furthermore, 102 patients (47%) had a blood vitamin C level below 11 µM/L, which is suggestive of scurvy (1718). Several studies conducted in developed countries have reported both vitamin C deficiency and scurvy (171819). Skin rash, poor dentation, chronic gingivitis, general myalgia, anemia, arthralgia, and peripheral neuropathy are suggestive symptoms of scurvy and as well as common findings among homeless patients. Moreover, vitamin C deficiency can aggravate symptoms of alcoholic liver disease such as bleeding, jaundice and malaise. It would be expected that many cases of subclinical scurvy among the alcoholic homeless are overlooked (4171819). In our study in fact, the admitted patients' lower vitamin C levels relative to those of the discharged patients suggested that acutely alcohol-intoxicated homeless patients requiring medical attention and admission to a hospital have lower vitamin C levels. For such patients, vitamin C supplementation should be considered.
Nonetheless, it is difficult to explain exactly why vitamin C deficiency is common among the homeless. What it is well known is that alcohol ingestion inhibits vitamin C absorption, and alcohol metabolism, in turn, consumes the body's reserves. Insufficient intake of vitamin C among the homeless also has been reported (813).
Several studies on smokers have reported deficiencies of several vitamins. More specifically, for example, an inverse relationship between tobacco exposure and plasma vitamin C level has been demonstrated, as have some independent effects of smoking on decreased plasma levels of vitamin C (20212223). In our present results, there were no definite differences in the blood vitamin levels between the smokers and nonsmokers (Table 3). Among the patients whose smoking information was available (n=112), most (n=90, 80.4%) were smokers; and, as other factors such as alcohol ingestion, malnutrition, and other relevant medical conditions were expected to influence the blood vitamin levels, it seems that the effect of smoking was masked.
Thiamine and other vitamin B deficiencies, relative to the case of vitamin C, are uncommon (91011). The mechanism of thiamin's conservation in homeless patients is uncertain. Possibly, due to serious concerns for prevention of Wernicke's encephalopathy in the treatment of alcohol-intoxicated patients, the present subjects had been administered thiamin supplementation on a previous ED visit (1024). Indeed, for decades now, social support programs such as include homeless shelters or nutritional support have been launched, and these might help to correct the nutritional imbalances typically suffered by homeless patients (25).
High vitamin B12 levels in the blood were relatively common among our patients (23%) (Table 2, Fig. 1). The median levels of the admitted tended to be higher than those of the non-admitted patients (871.0 [434.5-1,319.0] pg/mL vs. 600.5 [465-856.5] pg/mL), though the differences were not statically significant (P=0.053). High vitamin B12 levels also were more common among the admitted (n=14, 45.2%) than the non-admitted patients (n=36, 19.4%, P=0.04). Patients with liver cirrhosis showed higher vitamin B12 levels as well (1,179 [659-1,170] pg/mL vs. 713 [438.0-859.2] pg/mL, P<0.001) (Fig. 3). Some reports have indicated that high vitamin B12 levels are common in critically ill patients and are correlated with renal failure, malignancy, hematologic disease, infection, chronic liver diseases, and alcohol consumption (26272829). The exact mechanism of such increased blood levels is not certain, though a high vitamin B12 level can actually be a sign of functional vitamin B12 deficiency (2627).
There are some limitations to this study. First, clinical vitamin deficiency can be present even though the blood level is within the normal reference range. In fact, several studies have shown that there can be clinical symptoms of vitamin deficiency despite normal blood vitamin levels (30). However, in the present results, 17.5% of the vitamin B1 and 23% of the vitamin B12 levels were higher than the reference ranges. Vitamin supplementation for such patients should be reconsidered. Second, this study was a retrospective review of laboratory tests; as such, the levels of daily vitamin intake could not be obtained. Also, because almost all of the patients were in the acutely intoxicated state, detailed medical history taking was limited. Third, we did not conduct any full evaluation of scurvy. Such diagnosis is problematic, especially given the lack of any definite diagnostic criteria. Complicating matters further is the fact that most symptoms of scurvy are non-specific; for example, whereas gingival pathology and skin lesions are major indicators, the dental health of the homeless, in any event, typically is very poor, and skin problems also are common. Clinical follow up after vitamin C supplementation is essential for diagnosis of scurvy. Fourth, we did not evaluate other micronutrients, such as vitamins D and E. Recent studies have reported deficiencies of these vitamins in acutely and chronically ill patients as well as correlations with poor prognosis.
Finally, because this study was conducted in a single ED, and given that severely ill patients (ESI levels 1 and 2) were not included, generalization of the data will require very careful consideration. All of these limitations notwithstanding, this study is the first to evaluate alcohol-intoxicated homeless ED patients. To fully account for the limitations above-noted, a follow-up prospective multicenter study will be needed.
In conclusion, the incidence of vitamin C deficiency among acutely alcohol-intoxicated homeless patients in Korea is very high. Vitamin C supplementation should be considered for such patients in EDs. Vitamin B1, B12, and B6 deficiencies, by contrast, are less common than expected.




 XML Download
XML Download