

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the leading cause of death from gynecologic cancer worldwide (1). More than 70% of ovarian cancers are detected at advanced stage, because most patients at earlier, more curable stage have no specific symptoms. The 5-yr survival rate is about 80% to 90% for patients with stage I disease, whereas only 30% for patients with stage III or IV (2). Despite several trials to improve survival rates in patients with advanced ovarian cancer, the results were not satisfied (34). Therefore, early detection is the key to the successful treatment.
Unfortunately, effective screening tools for early detection of ovarian cancer have not been established yet (56). Although most gynecologic oncologists are using multimodality screening with transvaginal ultrasonography and CA125 in early detection of ovarian cancer, it is expensive and not as sensitive or specific as necessary (5,7,8). Risk of malignancy index (RMI), where M is menopausal status, U is ultrasound findings and C is serum CA125 level, is the most widely used tool for the detection of ovarian cancer. Patients with pelvic mass can be stratified into high and low risk groups according to RMI. In two prospective multicenter studies, a sensitivity and specificity of RMI was approximately 81 to 92% and 82 to 85% respectively (910). CA125, which is a key factor in the RMI system, has been so far the best-performing single tumor marker in early detection and prediction of prognosis of ovarian cancer. However, CA125 can be elevated not even in ovarian cancer but also in benign gynecologic and non-gynecologic diseases. Furthermore, 20% of ovarian cancer patients presented normal or only slightly elevated serum CA125, especially in early stage disease (1112). Recently, several new markers have been proposed and investigated for early detection of ovarian cancer. Among them, special attention has been focused on Human Epididymis-specific protein 4 (HE4), a precursor of human epididymis protein. A number of studies reported that HE4 protein is frequently over-expressed in ovarian cancers (1314). Specifically in a study for premenopausal women, HE4 was reported to offer superior specificity in discrimination of benign from malignant ovarian masses compared to CA125 (15). Based on a meta-analysis approach, recent guidelines have suggested that HE4 could be used as an aid in ovarian cancer diagnosis (16). Similarly, some authors have proposed the use of HE4 in combination with a symptom index and CA125 as an annual first-line screen for ovarian cancer (17).
In addition, other studies have proposed the use of a risk of ovarian malignancy algorithm (ROMA) in predicting ovarian cancer. ROMA calculates the probability of risk for ovarian cancer, by considering CA125, HE4, and the menopausal status of patients. By the combined use of both tumor markers, ROMA was expected to improve the sensitivity and specificity in patients with pelvic masses (1819). Some authors reported that ROMA had better diagnostic performance than the widely used RMI (20). In contrast, other authors suggested that there is no benefit from combining HE4 and CA125 in ovarian cancer screening (21,22,23). A prospective cohort study including 160 women consisted of healthy controls, benign diseases, and borderline tumors/adenocarcinomas of ovarian, tubal, peritoneal and endometrial origin, showed that there was no other detection benefit from RMI compared to HE4 alone or included in ROMA (23). Other prospective study, which includes 389 women with pelvic mass showed that HE4 and ROMA did not perform significantly better than CA125 (AUC for HE4 0.857, AUC for ROMA 0.898, AUC for CA125 0.877) (22).
There have been few data of HE4 and ROMA based on Asian population (2425). Recently, a prospective trial including 319 Japanese women (131 benign, 19 borderline, 75 malignant, and 94 healthy controls) reported that ROMA showed better sensitivity than CA125 and HE4 in the diagnosis of type I and II epithelial ovarian cancer (25). However, there have been no data based on Korean women.
Therefore, in this study, we aimed to compare CA125, HE4, and ROMA and evaluate the efficacy of each diagnostic tool in predicting epithelial ovarian cancer of Korean women.
MATERIALS AND METHODS
Patients
This is a prospective, multicenter clinical study conducted at Hallym University Medical Center in Korea (Dongtan Sacred Heart Hospital, Kangnam Sacred Heart Hospital, Chuncheon Sacred Heart Hospital, and Pyeongchon Sacred Heart Hospital). From December 2014 to April 2015, 90 Korean women with pelvic mass and 79 Korean women without pelvic mass (for control group) were consecutively enrolled. Exclusion criteria were as follows: 1) Women with known relapse of a previous cancer,2) Women with co-existence of cancer in other sites. Prior to surgery, all patients underwent pelvic ultrasonography (transvaginal and/or transabdominal). Then, the ovarian masses were removed surgically and examined by a pathologist specialized in gynecologic pathology. In cases with ovarian cancer, full surgical staging and optimal debulking (residual tumor less than 1 cm in diameter) was performed. If optimal debulking surgery was not possible, biopsy for diagnosis and staging followed by neoadjuvant cheomotherapy and interval debulking were suggested. The International Federation of Gynecology and Obstetrics (FIGO) criteria for epithelial ovarian cancer staging were used to classify the patients (26).
All patients were registered online data sheet. Clinical data (age, menopausal status, serum CA125 and HE4 levels, and ROMA), treatment information, and survival status are updated continuously.
Methods
Blood samples were collected within 2 weeks prior to surgery (in women with a pelvic mass)/or at visit of enrollment (in women without a pelvic mass). Serum CA125 and HE4 levels were determined using the fully automated chemiluminescent microparticle immunoassays (CMIA) on the Architect i2000 system (Abbott Diagnostics Division, Illinois, U.S.A), according to manufacturer's instructions, and appropriate controls were included in each run. ROMA was calculated using the following algorithms proposed by Moore et al. (18):
Then ROMA-value (predictive value) was calculated using the following equation:
Menopausal status was defined as absence of periods from more than 1 yr.
Statistical analysis
Clinical data registered in online datasheet were used for statistical analyses. Categorical variables were compared by Fisher's exact test or chi-square test as appropriate. Continuous variables were compared by t-test. The accuracy of HE4, CA125, and ROMA in discrimination of cancer from benign disease was evaluated by using the receiver operating characteristics (ROC) curve analysis. Overall and menopausal status subgroup ROC curves and areas (accuracy) for CA125 vs. HE4 vs. ROMA were plotted and compared using the chi-square test. For all statistical tests, P value less than 0.05 was considered significant. Statistical analyses were performed using SPSS for Windows (version 21.0, SPSS Inc., NY, USA) and Medcalc software (version 15.2.2, Portland, USA).
RESULTS
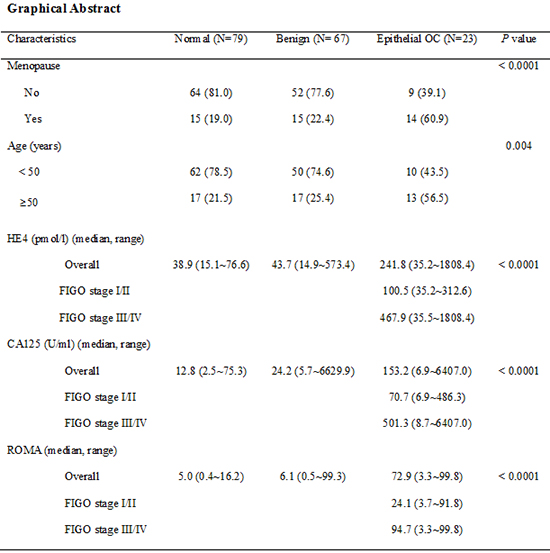
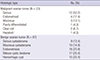
Among the 90 women with a pelvic mass, 23 were malignant and 67 were benign. There were no cases of borderline ovarian cancer during the study period. Women with menopause and older age (≥50 yr) were frequently observed in ovarian cancer group than others (Table 1). Also, serum HE4 and CA125 levels, and ROMA score were all significantly higher in ovarian cancer group than others (P<0.001) (Table 1). Among 23 cancer patients, 9 were stage I-II and 14 were stage III-IV. Subgroup analysis revealed that HE4 level and ROMA score in advanced stage (FIGO stage III-IV) ovarian cancer group were about 4 times higher that early stage (FIGO stage I-II) group (Table 1). Most frequent histologic type was serous adenocarcinoma in ovarian cancer group and mature cystic teratoma in benign ovarian tumor group (Table 2).
In ROC curve analysis, area under the curve (AUC) in discriminating ovarian cancer from benign ovarian disease was 0.755 for CA125, 0.859 for HE4, and 0.860 for ROMA, and there were marginally statistical differences among three markers (Fig. 1A; P compared to CA125; 0.0818 for HE4 and 0.0690 for ROMA). In sub-group analysis, AUC was 0.766 for CA125, 0.746 for HE4, and 0.749 for ROMA in premenopausal women (Fig. 1B). And no statistical differences were found. Similarly, in postmenopausal women, AUC was 0.729 for CA125, 0.838 for HE4, and 0.795 for ROMA and there were no statistical differences among three markers (Fig. 1C).
In the detection of benign ovarian tumor from normal population, AUC was 0.711 for CA125, 0.590 for HE4, and 0.587 for ROMA and there were marginally statistical differences among three markers (Fig. 2A; P compared to CA125; 0.0826 for HE4 and 0.0656 for ROMA). In sub-group analysis, AUC was 0.787 for CA125, 0.733 for HE4, and 0.818 for ROMA in premenopausal women, which showed no significant statistical differences among three markers (Fig. 2B; P compared to CA125; 0.6401 for HE4 and 0.6097 for ROMA). However, in postmenopausal women, AUC was 0.720 for CA125, 0.618 for HE4, and 0.620 for ROMA and there were marginal statistical differences among three markers (Fig. 2C; P compared to CA125; 0.0908 for HE4 and 0.0873 for ROMA).
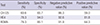
Suggested cut-off values for HE4 and ROMA determined by ROC curve analysis was 72.3 and 14.6, respectively. HE4 and ROMA provided better sensitivity, specificity, negative and positive predictive values comparing to CA125 (Table 3).
DISCUSSION
In this study, we aimed to prospectively assess whether preoperatively measured serum concentration of HE4 and ROMA score is superior to CA125 in the detection of ovarian cancer in Korean women with a pelvic mass.
Our data showed that both HE4 and ROMA score was not inferior to CA125 as an independent diagnostic tool in discriminating epithelial ovarian cancer from benign disease. Moreover, HE4 and ROMA offered higher sensitivity, specificity, positive and negative predictive values than CA125 in women with a pelvic mass.
HE4 and ROMA score has been in the limelight for early detection of ovarian cancer, which is generally detected in advanced stage disease. A number of data supports that HE4 seems to be more specific than CA125, which has low sensitivity in early stage ovarian cancer (1418,27,28,29,30,31,32). ROMA, which incorporates serum CA125 and HE4, and the menopausal status, has been also currently proposed as an effective diagnostic tool in ovarian cancer (1933). Moreover, HE4 and ROMA showed better accuracy than CA125 alone, in postmenopausal women (34).
In contrast, other studies showed no benefit of HE4 and ROMA (2324). A recent prospective study suggested that ROMA, and also HE4 alone, showed similar performance to CA125 alone in pre-menopausal women, but worse performance in postmenopausal women (22). In another retrospective study, HE4 was not superior to CA125 in predicting borderline ovarian tumors or presence of invasive implants (35).
These differences could be stem from the racial differences and related histologic types of ovarian cancer in study populations. Although data from Asian women is relatively rare, some studies suggested that the diagnostic role and appropriate cut-off values of HE4 and ROMA should be re-evaluated in Asian women with a pelvic mass. For an instance, Asian women showed a relatively higher incidence of mucinous epithelial ovarian cancer compared to Caucasian women and lower serum HE4 level (2436). A prospective, multi-centered study with patients from six Asian countries showed that median HE4 level in women with ovarian cancer was lower than the recommended cut-off (140 pM/L), which is based on studies in Caucasian populations (24). They used HE4 cut-off 70 pM/L for all women, which is similar to our cut-offs (72.3 pM/L for all women) (24). ROC curve analysis showed that ROMA had a better performance than CA125 in the detection of ovarian cancer (P value compared to CA125; 0.0102 for ROMA), which is similar to our data (24). In addition, they reported that ROMA showed a clear benefit in premenopausal women (24). ROMA offered improved specificity (87.4% vs. 63.2%) and positive predictive value compared to CA125 (34.69% vs. 16.8%), in premenopausal women (24). On the contrary, our data showed that menopausal status did not affect the performance of HE4 and ROMA in the detection of ovarian cancer. In addition, suggested cut-off values in pre- and post-menopausal women for HE4 (69.2 pM/L vs. 72.3 pM/L) and ROMA (15.1 vs. 19.3) in our data were almost same. It may be meaningless to use 2 cut-offs for pre- and postmenopausal women, since Moore et al. recently showed that HE4 increases with age, not with menopausal status (37). According to a cut-off suggested by ROC curve analysis, HE4 and ROMA score offered better sensitivity (78.3% and 78.3% vs. 69.6%), specificity (94.0% and 85.1% vs. 65.7%), negative (92.6% and 91.9% vs. 86.3%) and positive predictive values (81.8% and 64.3% vs. 59.0%) compared to CA125 in discriminating ovarian cancer from benign ovarian tumor.
There was limited literature about HE4 and ROMA algorithm in single-race Asian women. Specifically, there was only one prospective study for 159 Korean women, including 78 women with ovarian cancer (38). The authors suggested that ROMA score may provide higher accuracy for detecting ovarian cancer (87.5% sensitivity at a specificity of 93.8%) (38). But they compared serum CA125 only and ROMA score, not HE4 only, in predicting ovarian cancer.
In spite of small subjects including only 23 cancer patients, our data is worth focusing. This is the only prospective data comparing serum HE4, CA125 and ROMA scoring in the detection of ovarian cancer in single-race Asian women. In addition, we included normal population without pelvic mass for control group in our study. In our data, both HE4 and ROMA score showed better performances than CA125 for the detection of ovarian cancer in women with a pelvic mass, which suggested that HE4 and ROMA can be a useful independent diagnostic marker for epithelial ovarian cancer in Korean women.
Also, our data supported that those optimal cut-off values for serum HE4 and ROMA score should be fixed appropriately for Asian population. In addition, it may be re-considered to use 2 separate cut-offs for pre- and postmenopausal women. To clarify the diagnostic role of serum HE4 and ROMA in Asian women, more large-scaled prospective study will be required.



 XML Download
XML Download