

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As is the case worldwide, the disease burden of chronic disease is continually increasing in Korea (123). However, the quality of the treatment and management for chronic diseases remains low (45). In particular, the management quality in primary care medicine is at a relatively low level. For example, the rates of measurements of indicators of diabetes complications, such as glycosylated hemoglobin test, lipid profile test, and funduscopic examination, are lower in primary care clinics than in hospital-level facilities (6). Moreover, patient distrust of primary care and distortions of health-care delivery systems have caused many patients with chronic disease to prefer the services of hospital-level institutions (789).
As a key strategy for enhancing the management of chronic diseases in primary care clinics, the Korean Academy of Medical Sciences (KAMS) and the Korea Centers for Disease Control and Prevention have been jointly developing clinical practice guidelines (CPGs) for chronic diseases since 2011 (1011). CPGs for hypertension and diabetes were developed in 2013. Several CPGs for major chronic diseases will continually be developed. In this process, the first step should be deciding priorities. Under the constraint of a limited funding, priority setting and resource allocation are required. Moreover, the fair selection of subjects, on the basis of evidence, is of fundamental importance to promote the development of CPGs and encourage the applications for guidelines in clinical fields (12).
Prioritization is a systematic approach to allocating resources for creating the "best" health-care system, subject to a variety of demands and limited resources (1314). In addition, another strategy is to focus public attention and capabilities on key health issues (15). In decision making in complex health-care situations, a "reasonable side" and an "intuitive side" can be considered simultaneously when prioritizing alternatives for multiple criteria (1617).
By establishing a special committee for priority setting and surveying objective and subjective assessments, this study identifies the chronic diseases that need to be prioritized in the development of CPGs in Korea.
MATERIALS AND METHODS
Overall process
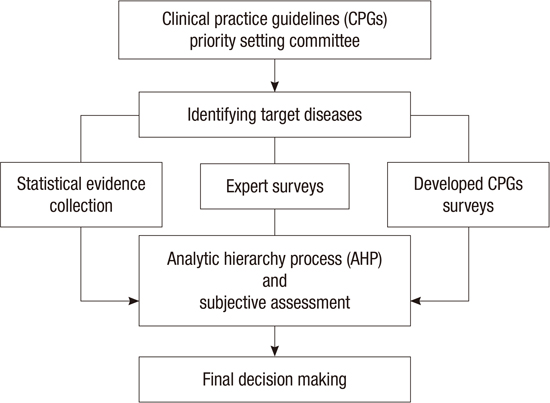
The prioritization was performed as follows (Fig. 1) : i) creating the CPG Priority-Setting Committee with representatives of 26 medical associations and CPG experts, ii) identifying the target chronic diseases, iii) collecting statistical data on those chronic diseases and examining the current developmental status of CPGs in Korea, iv) surveying the opinions of experts from the CPG Priority-Setting Committee by using the analytic hierarchy process (AHP) and a subjective assessment, and v) determining final priorities.
The CPG Priority-Setting Committee
The CPG Priority-Setting Committee was composed of experts representing the users and developers of CPGs. There were 36 members including primary care physicians from the Korea Medical Practitioners Association representing the end user, members of the CPG committee of KAMS, and experts on the methods of guideline development.
Identifying target chronic diseases
The prioritized targets among the chronic diseases were extracted by using the Global Burden of Disease (GBD) and the 2012 Health Insurance Statistics Yearbook (18). The GBD classifies the diseases and injuries into 291 causes, whereas the International Statistical Classification of Diseases and Related Health Problems 10th revision (ICD-10) classifies 22 classes, 267 categories, and 2093 subcategories. Among the 144 causes, those classified as noncommunicable diseases in the GBD were selected and matched with the ICD-10 categories. However, neoplasm, oral disorders, and hypertension and diabetes (the diseases for which CPGs are currently being developed by KAMS) were excluded. Finally, 41 chronic diseases were selected. Those diseases are the prioritized targets of this study.
Collection of statistical evidence and surveys of already developed CPGs
Prioritization in the development of CPGs for chronic diseases could provide standards for the fair distribution of resources in order to decrease the social burden of those diseases. Therefore, to reflect the impact of a chronic disease on the judgment of priority, condition-level criteria focused on the burden of the disease were selected (19). Four criteria were considered: prevalence rate, mortality, medical expenses, and disability-adjusted life years (DALYs). Statistical data for the numbers of patients and medical expenses of disease-specific ICD-10 codes by categories were extracted from the Health Insurance Statistics Yearbook. The mortality rate was extracted from the database of the National Statistical Office of Korea. DALYs were extracted, according to cause, from the GBD. The prevalence rate was applied to the number of patients as a proxy indicator. All data were normalized by using the z-score to enhance the comparativeness between the criteria. To identify the current developmental status of CPGs in Korea, a mail survey to 133 affiliated medical associations was conducted through KAMS. Data on the burden of disease and a list of available CPGs were provided to the committee for consideration in the prioritization process.
Expert surveys
The expert survey was performed in 2 ways: objective measurement methods with the AHP (objective assessment) and asking about subjective priorities for CPG development (subjective assessment). AHP is a multicriteria analysis performed to determine priority by classes after classifying the criteria. This method consisted of 4 steps. The first step was to create a decision model (2021). The AHP in this study comprised 3 levels (Fig. 2). Level 1 involved the ultimate goal of the AHP; that is, the ranking of chronic diseases for which there is a need to develop CPGs. Level 2 involved the 4 criteria to be considered when CPGs are chosen for chronic diseases. We would have also liked to include variability as a criterion; however, we could not find data to clarify the current situation in Korea. Therefore, the developmental status of CPGs was surveyed instead of the variability. Level 3 involved identifying the 41 target chronic diseases. The AHP analysis model in this study is described below.
The second step was to determine the relative priorities of the criteria by making a series of pairwise comparisons among them with Saaty's discrete 7-value scale method (20). The third step was to calculate the geometric mean of each criterion in the matrix to obtain an approximate eigenvector that is the weighted value of the 4 criteria. Finally, the fourth step was to apply the weighted values to the standardized status (the z-score) of the 41 diseases. Consequently, the final prioritized diseases were determined.
On the other hand, the subjective assessment was performed by asking about subjective priorities for CPG development. Each disease was evaluated on a 7-point scale in terms of priority for CPG development, and the priority order was selected by summing the scores from the evaluators. The experts ranked the priorities by disease, excluding those diseases in their medical field. Therefore, the results were unaffected by the specific interests of expert societies.
RESULTS
Target diseases and burden of disease
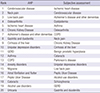
The 41 chronic diseases, their ICD-10 codes, and the burden of diseases are described in Table 1. Musculoskeletal diseases such as neck pain and osteoarthritis show a high prevalence and confers high medical expense but have low mortality rates. Although low in prevalence, cerebrovascular diseases present high DALY rates and high mortality.
Prioritizing by expert survey
Of the members of the CPG Priority-Setting Committee, 36 were surveyed with the AHP. Of them, 22 answered (61.1% response rate). The AHP assessment showed that among the criteria for measuring the burden of disease, high importance was placed on mortality and medical expenses (Fig. 3).
In both the AHP and subjective assessments, 7 diseases received an equal high priority: ischemic heart disease, cerebrovascular diseases, Alzheimer's disease and other dementias, osteoarthritis, neck pain, chronic kidney disease, and cirrhosis of the liver. The AHP showed that cerebrovascular diseases had the highest priority for CPG development; cardiovascular diseases such as ischemic heart disease and dyslipidemia were also ranked highly. The priority level of musculoskeletal disorders, such as neck pain, low back pain, and osteoarthritis, was also high. The subjective assessment showed that cardiovascular diseases such as ischemic heart disease, cerebrovascular diseases, and dyslipidemia had high rankings. The top 20 diseases that received a high priority are shown in Table 2.
DISCUSSION
Recently, CPGs in various areas have been developed through the voluntary efforts of academic societies. However, despite the high burden of diseases and the clinical importance of CPGs, several major chronic diseases do not have CPGs (2223). Moreover, some of the many CPGs that have been developed already require revision. By November 2013, there were 141 CPGs in Korea (see Table S1). If the first edition of a CPG and its revised version are counted as 1, there are now 125 CPGs that have been developed by 76 academic societies or institutions in Korea. Of them, 83 CPGs are related to chronic diseases. Moreover, among those CPGs for chronic diseases, 40 guidelines had been developed in the last 5 yr (since 2010). Considering the rate of the production of new evidence in medicine and the worsening of the burden of chronic diseases, the need for developing more CPGs for chronic diseases is becoming increasingly pressing.
Among the criteria used to measure the burden of disease with the AHP, medical expenses and mortality were considered of high importance. Diseases with a high burden, such as cerebrovascular diseases, ischemic heart disease, musculoskeletal disease, and dyslipidemia, received high rankings that indicate the need for the development of CPGs.
Cerebrovascular diseases and ischemic heart disease are serious causes of death in Korea, and the medical expenses and numbers of patients with these diseases are very high. Furthermore, when the major risk factors-hypertension and diabetes-are considered, the disease burden becomes even greater (24). However, among the guidelines developed since 2010, only 13 have targeted cerebrovascular diseases and only 2 have a focus on ischemic heart disease. Furthermore, unfortunately, although many CPGs have been developed in recent years, they have focused on use in tertiary hospital institutions. CPGs reflecting the clinical features in primary care, the values and preferences of patients, and the environment of primary care institutions for the management of chronic diseases are insufficient. CPGs for disease prevention, lifestyle management, and follow-up care after the acute period of disease should be developed. For example, CPGs about primary and secondary prevention, screening, mild stable angina management, and indications for referring to tertiary institutions would be useful.
The situation for musculoskeletal disorders is even more serious. To date, despite the high burden of musculoskeletal disease, only 2 of such diseases-osteoporosis and rheumatoid arthritis-have CPGs in Korea. Given the high level of disease burden and the high variability in the behavior of health-care providers in musculoskeletal disorders (25), the development of more CPGs is urgently required. In addition, there is a pressing need for the development of guidelines on dementia, chronic renal failure, liver disease, asthma, and chronic obstructive pulmonary disease. Owing to the increase in the elderly population, the prevalence of dementia continues to increase (26). However, there is only one guideline related to dementia, which was developed in 2009, and it only covers disease diagnosis. Thus, the development of new guidelines for dementia is urgently needed, for application in various areas, including a set of detailed services about the prevention of disease, behavioral intervention, and pharmacological therapy, among others.
Moreover, the CPGs to be developed for those diseases are also expected to be consistent with national policies, in which the importance of cerebrovascular diseases, ischemic heart disease, and dementia has been increasing consistently. Those diseases are the main targets of "Health Plan 2020," and risk factors such as smoking, drinking, exercise, and nutrition are the subjects of active management in the National Cerebrovascular Management Project, based on the National Health Promotion Act (27). In the case of dementia, the Dementia Management Act was enacted in 2012 and provides a legal foundation for prevention, early detection, and follow-up. Moreover, a dementia-screening program is being implemented throughout the country as a national policy. Furthermore, since the introduction of long-term care insurance, the frequencies of diagnosis, treatment, and care management by primary care physicians have increased (28). However, there is as yet no guideline for these physicians, which makes it difficult to provide appropriate services
In this study, we found a high need for CPGs for chronic diseases in Korea. Considering the rate of the production of new evidence in medicine and the worsening of the burden from chronic diseases, the need for developing more CPGs for more chronic diseases is becoming increasingly pressing.
In most countries with advanced CPG development, the establishment of public-private partnerships (PPPs) has been emphasized to develop the most reliable guidelines at a high level. Furthermore, this ensures the participation of various stakeholders in the development of CPGs and their quality control, leading to a social consensus for any conflict resolution caused by the CPGs (2930). The United States has mandated the use of PPPs in developing CPGs (31). In Australia, the principles of development and a social consensus about the legal status of CPGs have been developed jointly by medical societies and the government (32). In Korea, however, most of the developmental activities depend on professionals. KAMS has led the development of CPGs, whereas the government's role has been confined to providing financial support. To develop high-quality CPGs, and to enhance implementation in practice, collaboration between professionals and the government is essential. PPP for financing, granting official status to accredited CPGs, and creating a favorable environment for implementation could lead to the development of CPGs with high quality.




 XML Download
XML Download