

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Korea has been noted for high prevalence of alcohol use disorders (AUD) and exceptionally high male-to-female ratio of AUD prevalence (12) based on the results of a national epidemiologic survey conducted in 1984 (3). The lifetime prevalence of AUD was 42.9% in men and 2.6% in women, resulting with a male-to female ratio of 16.5 (3). In total population, the prevalence of AUD was 23%, which is higher than reported figures of other countries (1) such as the United States (17%) (4), Taiwan (7%) (5). The fact that the 1984 Korean study was conducted with the same methodology used in Epidemiologic Catchment Area (ECA) study in the US (6) using the Diagnostic Interview Schedule (DIS) (7) allowed for direct comparisons with the DIS-based data from other countries.
After 15 yr, a regional survey was conducted in 1999 among Korean community residents using the Composite International Diagnostic Interview (CIDI) (8) to assess Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) disorders. In the study, the prevalence of AUD in total population was decreased from 23% in 1984 to 15.6% in 1999. The male-to-female ratio of prevalence dropped from 16.5 in 1984 to 5.8 in 1999 (2). Although the differences in the diagnostic system could have affected the results of the comparisons between the 1999 survey and the 1984 survey (2), the trend of narrowing gender gap in AUD was consistent with the reports in the United States (9). During the same period in the United States, male-to-female ratio of prevalence for alcohol dependence (AD) decreased from 5.17:1 in the 1982 ECA study (10) to 2.45:1 in the 1990-92 National Comorbidity Survey (NCS) (11).
More recently, Grant et al. (12) compared the National Longitudinal Alcohol Epidemiologic Survey (NLAES) (13) conducted in 1991-1992 and the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) (14) conducted in 2001-2002. They found that the gender ratio had further diminished from 3.09 to 2.72 for AA and from 2.45 to 2.34 for AD, although the decrease between NESARC and NLAES was more gradual than the change between ECA and NCS (12). And additionally, the result from National Survey on Drug Use and Health (NSDUH) conducted by Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality (SAMHSA) also showed even narrowed gender ratio of 2.0 for 12-month alcohol use disorder(male; 9.4%; female 4.7%) in 2013 (15).
Meanwhile, in 2001, the first nation-wide epidemiologic survey for DSM-IV mental disorders in Korea, the Korean Epidemiologic Catchment Area (KECA) (16) survey was conducted. A cross-cultural comparison of the results of KECA in Korea and NESARC in United States revealed greater gender gap in Korea (17). The gender ratios of prevalence for abuse and dependence among Koreans (AA, 5.83; AD, 4.87) were much greater than their American counterparts (AA, 2.57; AD, 2.21).
Over the 10 yr since 2001, the Korean society had experienced a rapid change in sociocultural environment regarding gender. More and more women receive higher education and participate in the workforce in Korea. College enrollment rate for women increased from 65.4% in 2000 to 80.5% in 2010, surpassing the rate of men, which was 77.6% in 2010. Employment rate for women has increased from 38.3% in 2000 to 41.1% in 2010 (18). More specifically, the employment rate for women in their 30s was 54.8%, 40s was 65.3%, and 50s was 57.9%, indicating that more than half of the female population were active participants in the economy.
As these changes would inevitably affect the epidemiology of AUD, a new research endeavor to evaluate the current trends in gender difference in AUD in Korea is necessary. Understanding true changes in prevalence over time may be crucial for research on the etiology of AUD (19). Since the distribution of genotypes does not vary within such a short period as a decade, shifting prevalence suggests changes in the level of environmental risk (12). In addition, the evaluation conducted in Korea would generate information about not only secular change, but also cross-cultural difference. The data from WHO World Mental Health Survey reported substantial cross-cultural variation in substance use disorders by gender (20). Keyes et al. (9) remarked that studies about birth cohort effect and gender difference were focused in the Western countries and that data from a broader cultural framework are needed.
However, few previous studies about change of gender differences for AUD have been conducted in Asia. Only some epidemiologic surveys conducted in China and Japan have suggested the trend of narrowing gender gap. In Beijing, gender ratio of lifetime prevalence of AD decreased from 48.3 (men 2.9%, women 0.06%) in 1991 (21) to 19.5 (men 7.8%, women 0.4%) in 2008 (22). In Japan, gender ratio of lifetime prevalence of AUD was 11.07 (men 15.5%, women 1.4%) in a nation-wide survey conducted between 1997 and 1999 (23). The ratio was reported as 5.07 (men 7.1%, women 1.4%) in more recent study conducted from 2002 to 2005 (24). However, these direct comparisons of these surveys are problematic due to the differences in diagnostic system and methodologies used in those surveys. In the case of Beijing, DIS was used to generate DSM-III diagnosis in 1991 (21), while CIDI 1.0 was used to make DSM-III-R diagnosis in 2008 (22). Japanese studies also used different diagnostic systems of DSM-III-R in 1999 (23) and DSM-IV in 2005 (24). Hence this study is the first report of direct comparison to analyze secular change of the gender difference in AUD in Asia. This study may provide a foundation for further research endeavor on AUD in other Asian countries and also among Asian immigrants in other parts of the world. The information on changes in AUD would also be helpful for policy makers because they can find potentially vulnerable groups and highlight the need for focused planning (12).
This study compared the results of the most recent national survey, the 2011 Korean Epidemiologic Catchment Area study (KECA-2011) with the results of KECA in 2001 to investigate the change in gender difference in DSM-IV alcohol abuse (AA) and alcohol dependence (AD) in Korea. Since the methods used in KECA-2011 were very similar to those used in the KECA survey, direct comparison is possible. The authors hypothesized that gender gap in alcohol use disorders would have decreased in 2011 compared to 2001, consistent with findings from United States.
MATERIALS AND METHODS
Study design and population
As the KECA and the KECA-2011 were nation-wide surveys for mental illnesses, the target population consisted of community-dwelling adults in Korea while excluding institutionalized individuals. Both surveys used multistage, cluster sampling method based on the population census of the Korean National Statistical Office in 2000 and 2010. The catchment areas for sampling were not the same, but very similar between the two surveys. Further details concerning the designs and methods of the KECA survey can be found elsewhere (16).
In 2001, the KECA survey was conducted across 10 catchment areas during the period between June 1 and November 30 (16). In 2011, the KECA-2011 survey was conducted across 12 catchment areas between July 19 and November 16 (25). Face-to face interviews were administered to community residents aged 18-64 yr in 2001 (n=6,220) and to those aged 18-74 yr in 2011 (n=6,022). For direct comparison, only respondents who were 64 yr old or younger were included in the analysis from the 2011 data (n=4,894).
Measures
To assess DSM-IV disorders, the Korean version of Composite International Diagnostic Interview (K-CIDI) (26) was administered to all subjects by trained interviewers in both surveys. The CIDI (8) is a fully structured diagnostic interview designed to produce standardized psychiatric diagnoses in various cultures. To gain reliable information for each diagnostic criteria of DSM-IV, the questions in CIDI were designed for laymen to understand and answer easily. For example, 'a great deal of time is spent in activities necessary to obtain alcohol, use alcohol, or recover from its effects' which is one of the diagnostic criteria of AD is questioned as "Was there ever a period in your life when you spent a great deal of time drinking or getting over the effects of alcohol?". The answers are assessed via computer algorithm to produce diagnosis. The K-CIDI was validated by Cho et al. (26) according to the World Health Organization (WHO) guidelines (27).
Statistical analysis
Data were adjusted to approximate the national population contributions of age and gender using weight values that were calculated according to the population census of 2000 and 2010 (18). To assess gender difference in prevalence and risk, the male-to-female prevalence ratios and odds ratios (OR) for AD and AA in each year and in each age group were calculated. To compare the data of the two national surveys, logistic regression was conducted in each age group by gender. OR for alcohol abuse and dependence in 2011 were calculated using the 2001 group as reference. SPSS 18th (Polar Engineering and consulting, 2009) was used for the analysis.
Ethics statement
The study protocol was approved by the institutional review board of the Seoul National University Hospital (IRB No. 1104-092-359). All the subjects were fully informed about the aims and methods of the study before completing the interview. Informed consent was obtained prior to participation.
RESULTS
Table 1 presents the socio-demographic profiles of the participants in 2001 and 2011. The proportion of males was larger in 2011 than in 2001. Compared to the respondents in 2001, the survey respondents in 2011 included more people over 50 yr of age, more people with higher education, fewer people who were married, and fewer people who were employed.
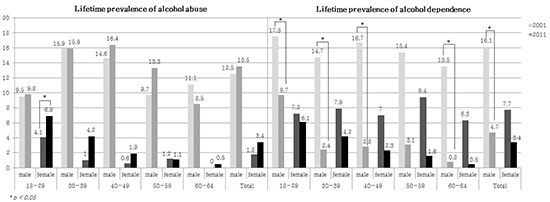
Male-to-female prevalence ratios and odds ratios were calculated for lifetime alcohol abuse and dependence in each survey year, in each age group (Tables 2, 3). While both alcohol abuse and alcohol dependence were still more prevalent among men than in women in all age groups, almost all groups showed a decrease in male-to-female prevalence ratios and odds ratios. In terms of prevalence, the male-to-female ratio had decreased in AA (from 6.94 to 3.97) and in AD (from 3.43 to 2.26) between 2001 and 2011. The male-to-female odds ratio had also decreased in AA (from 6.41 to 4.37) and AD (from 3.75 to 2.40). Though the 50-59 age group showed an increase in the male-to-female prevalence ratio for AA and AD after the interval of 10 yr, after adjusting for demographic factors such as marital status, employment, education year, the male-to-female OR decreased in AA (from 10.06 in 2001 to 9.79 in 2011) and AD (from 8.96 in 2001 to 6.84 in 2011).
In the case of the age group of 18 to 29 yr, the odds of men for AA went from being 2.49 times the odds of women in 2001 to being only 1.59 times the odds of women in 2011. Likewise, the odds of men for AD went from being 1.61 times the odds of women in 2001 to being only 1.38 times the odds of women in 2011. No significant difference was found in the risk of AA and AD between men and women in 2011 in this age group. The age group of 30 to 39 yr also showed a similar pattern. In 2001, the odds of men for AD were 4.02 times the odds of women, but there was no statistically significant difference between men and women in 2011 in risk of AD (Tables 2, 3).
To evaluate whether the changes of lifetime prevalence between 2001 and 2011 are statistically significant, the 2011-to-2001 odds ratios for AA and AD were calculated by gender in each age group (Table 4). In the case of men, the odds of experiencing AA did not change significantly between 2001 and 2011. On the other hand, they were less likely to experience AD in 2011 than they were in 2001. In men aged 40 to 49 and 60 to 64, odds for alcohol dependence in 2011 were less than half the odds than in 2001 (OR: 0.33, 95% CI 0.21-0.51; OR: 0.38, 95% CI 0.18-0.80). The change in risk for AD between 2001 and 2011 were insignificant (P=0.063) only in the case of the men in their 50s. In the case of women, the odds of experiencing AA increased significantly in 2011 for females in the 30-39 age, which were 2.13 times the odds in 2001. Also, the odds of AA for females in the youngest age group (18-29) in 2011 were 1.68 times the odds in 2001, approaching significance (P=0.053).
In short, the risk for AA had increased in young women while risk for AD had decreased in men between 2001 and 2011. These results indicate that the decrease of gender gap in AA was due to increased prevalence in women, while the change in AD was largely due to decreased prevalence in men.
DISCUSSION
This study found that gender differences in lifetime prevalence of AA and AD had decreased by 2011 compared to 2001 in Korea, as the researchers had hypothesized. The gender ratio of prevalence for AA decreased from 6.94 in 2001 to 3.97 in 2011 and the reason for this change was increase in AA among women. In contrast, decrease of AD among men contributed to decreased gender ratio in AD of from 3.43 in 2001 to 2.26 in 2011. In addition to the prevalence, the male-to-female odds ratios had also decreased for AA (6.41 to 4.37) and AD (3.75 to 2.40). The gender gap was the smallest in the youngest age group (age 18-29). The significant gender gap between men and women in the risk of AA and AD had disappeared by 2011 for young adults. Women had as much risk as men for AA in ages 18-29 and for AD in ages 18-39 in 2011.
These changes are consistent with the previous reports of narrowing gender gap in comparison with NLAE (13) in 1991-1992 and NESARC (NIAAA) in 2001-2002 in the United States (1228). However, the patterns are different between the United States (28) and Korea. The most remarkable difference is that the secular decrease of gender ratio was much steeper in Korea. In the United States, the gender ratio decreased from 3.09 to 2.72 for 12-month AA and from 2.45 to 2.34 for AD, while the Korean data reported that gender ratio decreased from 6.94 to 3.97 for lifetime AA and from 3.75 to 2.4 for lifetime AD. Also, the pattern of changes for AUD was more markedly different by gender in Korea. While AD decreased significantly among men and insignificantly among women in both countries, Korean men showed steeper decline. Among all age groups by gender, only Korean women in their 30s showed increased prevalence of AD, although the change was not statistically significant. In case of AA, AA had significantly increased both in men (4.67%-6.93%) and women (1.51%-2.55%) in the United States. In Korea, although AA had slightly increased in both sexes, the increase of AA was only significant in young women. Additionally, the gender gap and the prevalence varied greatly by age in Korea. The gender ratios of prevalence were 17.0 for AA and 12.6 for AD in the oldest age group (age 60-64) of 2011, which are very close to the figures for the total population in 1984, where they were 16.85 for AA and 20.4 for AD. On the other hand, the youngest group (age 18-29) of 2011 showed very low gender ratios of 1.42 for AA and 1.18 for AD. The prevalence was also remarkably different by age, especially in women. A comparison between the women aged 18-29 yr and women aged 60-64 yr showed striking differences in prevalence for AA (6.9% vs. 0.5%) and AD (6.1% vs. 0.5%).
To explain this steep decrease of gender gap, socio-cultural factors should be considered. WHO's world mental health survey (WHO WMHS) had linked the shrinkage of gender gap in recent cohorts for substance use disorders to variation in gender role traditionality by nation. The greatest reductions in the gender gap were reported among countries where women's roles have shifted the most from traditional to autonomous (20). The traditional Korean society had very rigid gender roles based on Confucianism, which had even set "the distinction between husband and wife" as one of the five fundamental moral disciplines in human relationships. Confucian principles imposed strict restrictions on social activities of women and expected them to devote themselves in the service of their family. In contrast, men were expected to actively pursue successful careers, engage in profitable endeavors, and socialize with peers, which involved much social drinking. Accordingly, the Korean society held two distinctive sets of values and attitudes toward men and women's drinking behavior (29). For women, opportunities for social drinking were practically nonexistent and drinking was considered as an immoral and insolent behavior, while for men, drinking alcohol was allowed, encouraged, and even enforced in some social contexts. Since alcohol was a social lubricant, and the consumption of alcohol is considered essential to many business and social gatherings (29), rejecting alcoholic drinks could be seen as rude and sometimes as an indication of social ineptness. In addition, heavy drinking was often associated with masculinity, encouraging men to drink as much as they can in social gatherings to prove their masculinity.
However, the social environment concerning gender has been changing in Korea. As more and more women break out of traditional gender roles and hold similar social positions as men, traditional expectations on gender roles are changing. As women are taking on roles that had been traditionally considered for men, experiencing the same kind of stress, and going through the same circumstances as men, they may have extended this imitation effect to susceptibility to AUD. Just as men participated in social drinking for their own careers, women who ventured forth to the previously male-dominated society of the workforce started to participate in social drinking as part of their career fulfillment. In addition to the correlation between drinking behavior and occupational subcultures (30), the increase in economic power for women facilitates their purchasing power for alcohol (31). Furthermore, the stigma associated with drinking behavior among women may have been reduced in recent years (32). Compared to the past when Confucian gender distinction had rigidly restricted alcohol consumption for women, Korean women today are much freer to drink alcoholic beverages. The decreased stigma and increased accessibility of alcohol may allow drinking become more popular as a coping strategy for stress in women. These changes are thought to attribute the increase of AA in Korean women.
The decrease of AD in Korean men could also be associated with socio-cultural changes. The Korean public had a high tolerance for drunkenness and mistakes made while drunk (217). This high tolerance was only for men and considered to be one of the key reasons for the much higher prevalence rate of AUD among Korean men than men in other Asian countries. Recently, the norm of the Korean society has shifted toward disapproving the serious problems associated with heavy drinking (2). The government had started a campaign against the notorious drinking culture to reduce socioeconomic loss resulting from excessive drinking in 2006. The penalties for drunk driving are becoming heavier and heavier since 1995. Since 69.6% of total households had individual transportation such as a car in 2010 (18), the increased automobile use has also impacted the drinking habits of the public (2). In 2010, the police declared to deploy intensive control of "Joo-pok", which means violence in drunken state. As the public are more informed of the hazards by heavy drinking, its association with negative outcomes like loss of self control, health problem and addiction is increasing instead of positive ones like social competence. Such socio-cultural change has probably contributed to the steep decline of gender difference.
The strengths of this study include the inclusion of a large pool of respondents on a national scale and the high reliability of AUD diagnosis by a systematic diagnostic tool, the CIDI. The CIDI is expected to lower defensiveness in responses as it asks about behaviors pertaining to diagnostic criteria and has a low false-positive rate because of its rigorous diagnostic criteria. The possible error due to difference in methodologies is minimalized as this study is a direct comparison of two similar surveys that used the same diagnostic tool and sampling method. Similar teams of researchers were involved and both studies used the population census of each year as a sampling frame. While the survey did not follow up on the same cohorts, the populations represented by the respondents are likely to be similar to each other as they were recruited from similar catchment areas representing each province of the country. Consequently, the resulting evidence provides the strongest support that is realistically possible from a cross-sectional study. The findings of this study may contribute valuable insight into the cross-national epidemiological distribution of AUD and its relation with socio-cultural factors and gender differences.
The current study is not without limitations. Firstly, self-report measures are susceptible to memory bias, which can result higher prevalence in younger population. However, because the participants were below 65 yr old, the likelihood of memory bias resulting from decline in cognitive ability is low. Also, the bias alone cannot explain the difference in gender gap by age group and the change between 2001 and 2011. Secondly, it is possible that changes in social norms caused the young women to be more open to disclosing their personal problems and more aware of alcohol-related problems than older adults. However, the CIDI does not ask whether the respondent has a disorder or a problem, but uses neutral questions about behaviors pertaining to diagnostic criteria, which would have helped reduce errors associated with defensiveness. More research would be necessary regarding response attitude in self-report measures.


 XML Download
XML Download