

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) remains a huge health burden worldwide (1). The currently recommended first-line treatment for TB is a regimen of isoniazid (INH), rifampicin (RMP), pyrazinamide (PZA), and ethambutol (EMB) for 2 months, followed by 4 months of INH and RMP and/or EMB (2, 3). Hepatotoxicity is one of the most frequent and serious adverse effects of anti-TB medications and may reduce treatment effectiveness by compromising treatment regimens (4, 5). Among the first-line quadruple therapy drugs (INH, RMP, PZA, and EMB), INH, RMP, and PZA are metabolized mainly by the liver, and therefore, are potentially hepatotoxic. The incidence of anti-TB drug-induced hepatotoxicity (DIH) during standard multidrug TB treatment has been reported to be between 2% and 28%, depending on the definition of hepatotoxicity and the population studied (5, 6). However, the biochemical mechanism and pathogenesis of DIH remain unclear for the most offending drugs. Therapeutic drug monitoring (TDM) during TB treatment allows the clinician to make informed decisions in cases involving slow response to treatment, drug-resistant TB, drug-drug interaction risks, or severe underlying diseases (7). However, whether DIH will develop more frequently with increasing serum drug levels is questionable. There are few reports on the direct correlation between basal serum drug levels and DIH, as it has not been well studied. RMP plasma levels were higher in cases with DIH than in controls and independently predicted subsequent development of DIH, according to one recent report (8). The slow acetylator status of INH metabolites may be a risk factor for anti-TB DIH (9, 10). Varying serum INH levels due to the different slow acetylator status may be a cause of hepatotoxicity. PZA has been shown to induce greater hepatotoxicity than other first-line anti- TB drugs (3, 11). Although the incidence of PZA-induced hepatotoxicity decreased considerably after reducing the recommended standard dose, PZA is still considered the most frequent cause of anti-TB DIH (11, 12, 13, 14). However, little is known about the serum levels of anti-TB medications and the development of hepatotoxicity in TB. The aim of the present study was to evaluate the association between the basal serum levels of anti-TB drug and the development of hepatotoxicity.
MATERIALS AND METHODS
Study subjects and procedures
This study was performed retrospectively at Seoul National University Bundang Hospital, a tertiary hospital in Korea. Patients diagnosed with TB were enrolled in the study and patients received anti-TB medication daily for at least 5 days before serum anti-TB drug level measurements. Patients aged less than 16 yr; with chronic kidney disease (GFR<60 mL/min/1.73 m2) or chronic hepatic dysfunction; human immunodeficiency virus (HIV) co-infection, acute viral hepatitis, or suspected malabsorption (e.g., gastrointestinal disease or diarrhea); and pregnant women were excluded from the study. The anti-TB drugs were all single drug products and administered daily dose were INH 300 mg, RMP 450 mg, EMB 800 mg, and PZA 1,000 mg in patients' body weight ≤50 kg, and INH 300 mg, RMP 600 mg, EMB 1,200 mg, and PZA 1,500 mg in patients' body weight >50 kg by daily dose guideline of the Korean Academy of Tuberculosis and Respiratory disease (15). Adherence or any drug adverse events was monitored and evaluated by doctor thoroughly every one month. Pharmacokinetic sampling was performed 2 hr after drug ingestion to estimate peak concentrations of the 4 drugs (INH, RMP, EMB, and PZA) and their 2 major metabolites (acetyl-INH and 25-desacetyl-RMP). The serum was separated and then frozen at -70℃ within 1 hr after the sample was obtained according to the published recommendations until required for analysis (7, 16). Pharmacokinetic analyses were performed using liquid chromatography-tandem mass spectrometry (17). The following target ranges of peak plasma concentrations for the 4 drug were defined on the basis of published reference ranges that have been evaluated and validated worldwide (7, 18): INH, 3-6 µg/mL; RMP, 8-24 µg/mL; PZA, 25-50 µg/mL; and EMB, 2-6 µg/mL.
Definition of drug-induced hepatotoxicity
All patients with TB underwent a liver function test (LFT) prior to receiving therapy and liver chemistry tests were performed on a monthly basis after the initiation of anti-TB treatment. For this study, hepatotoxicity due to anti-TB drug treatment was defined as the following criteria: 1) serum aspartate aminotransferase (AST) and/or alanine aminotransferase (ALT) levels >5 times the upper limit of normal (ULN; 40 IU/L) or >3×ULN, with clinical symptoms such as nausea, vomiting, abdominal pain, jaundice, or unexplained fatigue; 2) Absence of serological evidence of infection with hepatitis A, B, C or E (6, 15); 3) Normalization or at least a 50% improvement in abnormal liver chemistry results after withdrawal of anti-TB drugs (19). If LFT abnormality had occurred, viral serology tests (immunoglobulin M for hepatitis A virus, immunoglobulin M for hepatitis B core antigen) were performed to exclude acute viral hepatitis. History of alcohol use, herbal medication or other concomitant medication was intensively examined. We held INH, RMP, PZA if abnormal LFT results were reported and after normalization of LFT, re-challenged RMP or INH first and then PZA in order with monitoring LFT. We also evaluated patients with mild LFT abnormality, which was defined as an increase in serum AST or ALT levels from 60 IU/L to 3-fold the upper reference values after the initiation of anti-TB medication. Basal serum drug levels and the number of patients whose serum drug levels exceeded the reference level for each drug, and other clinical characteristics already reported to be risk factors for DIH such as age, sex, creatinine clearance, HBV carrier status were compared based on the development of hepatotoxicity.
Statistical analysis
Variables are represented as mean±SD (standard deviation) if normally distributed, and statistical significance was defined as a P value<0.05. In continuous variables, independent t-test was applied. Chi-square and Fisher's exact tests were used to compare categorical variables with hepatotoxicity. Additionally, to compare each TB drug concentration with the grade of hepatotoxicity, ANOVA was applied. Statistical analyses were performed using SPSS version 12.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 307 patients were treated with anti-TB chemotherapy and followed up with TDM between June 2006 and February 2010. The number of patients excluded from the study was 112. An additional 7 patients were lost to follow-up lower than 8 weeks after anti-TB therapy, 6 died of other causes, 5 were found to have nontuberculous Mycobacterium infection rather than TB, 10 had underlying abnormal liver chemistries, and 31 received medicine under a separate dosage schedule. For 53 patients, no data about PZA concentration were available due to the TDM schedule (they took PZA after meal). Finally, 195 patients were included in this study (116 men and 79 women) (Fig. 1). The median age was 46 yr (range, 16-92 yr). Patient characteristics and microbiological results are summarized in Table 1. The baseline serum concentrations of the 4 drugs were estimated at median 7 days (range 5-76) from the diagnosis of TB and suggested normal distributions. Among the 195 patients, 17 (8.7%) developed hepatotoxicity, and their mean AST/ALT values (mean±SD) were 249±229/249±250 IU/L. Adverse effects involving the gastrointestinal system (9.7%) and skin (7.7%) were the other frequently observed symptoms. The median interval between the initiation of anti-TB therapy and onset of hepatotoxicity was 41 days (range, 13 to 263 days). Among the 17 patients who developed hepatotoxicity, 5 were excluded for having anti-TB DIH. Acetaminophen (2 patients) and alcohol (2 patients) were the other putative causes of hepatotoxicity, and viral hepatotoxicity was presumed to be the cause in 1 patient. Ten patients were assumed to have PZA-induced hepatotoxicity because their liver enzyme abnormality normalized after the discontinuation of PZA and reintroduction of RMP and INH. INH or RMP was suspected to be the cause of hepatotoxicity in 2 patients because the liver enzyme levels increased again after the reintroduction of INH or RMP. The median latent period for developing DIH was 37 days (range 13-112) in anti-TB DIH group. It was median 28 days (range 0-107) from the day of TDM sampling.
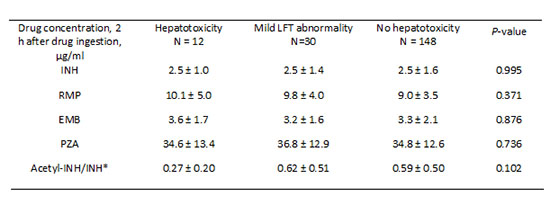
When we compared the serum anti-TB drug concentrations according to the presence of hepatotoxicity after excluding the 5 patients with other causes of hepatotoxicity, no significant differences in the serum drug levels were observed between the 2 groups (Table 2). Furthermore, no difference was found between the 2 groups when we analyzed the number of patients whose serum drug concentration level exceeded the reference level for each drug; 2 patients receiving PZA and 2 receiving EMB had serum drug levels higher than the reference range in the hepatotoxicity group. Similarly, in terms of factors that are known to increase the risk of hepatotoxicity, such as age, sex, and hepatitis B or hepatitis C carrier status were not significantly different between the 2 groups. However, the metabolic ratio of the plasma acetyl-INH to INH levels 2 hr after drug ingestion was significantly lower in the hepatotoxicity group than in the non-hepatotoxicity group (P<0.001).
Thirty other patients showed mild LFT abnormality, as defined previously (60 IU/L≤serum AST or ALT level<120 IU/mL). They were all asymptomatic and their therapy schedules were not interrupted due to increased LFT results. Their mean AST and ALT levels (mean±SD) were 66±24 IU/L and 76±20 IU/L, respectively, and their serum anti-TB drug levels were not significantly different from those of the non-hepatotoxicity group (Table 3).
DISCUSSION
This study showed that neither the serum anti-TB drug concentration, nor the proportion of patients whose serum drug level exceeded the reference level for each anti-TB drug investigated, were different among the groups (hepatotoxicity group, mild LFT abnormality group, and non-hepatotoxicity group). In this study the incidence of DIH was similar to the rates reported in previous studies (5, 6, 20, 21). Several risk factors for anti-TB DIH, such as old age, female gender, malnutrition, alcoholism, underlying liver disease, extensive pulmonary parenchymal disease, and HIV infection, have been reported in previous studies (5, 6, 22, 23). The findings obtained in this study were inconsistent with these known risk factors. This discrepancy probably resulted from the fact that patients with risk factors and comorbidities were strictly excluded to minimize the influence of other risk factors resulting in the development of DIH in the present study. The major strength of this study was the direct measurement of serum anti-TB drug levels after starting anti-TB therapy. Furthermore, the diagnosis of anti-TB DIH and the causality assessment were performed after a strict review.
The biochemical mechanism and pathogenesis of DIH are not fully understood. For most TB drugs, the relationship between dose and toxicity is unknown, except for hepatotoxicity being associated with high-dose PZA (>40 mg/kg daily) (24). However, recent antimicrobial pharmacokinetic-pharmacodynamic studies have suggested that PZA doses that are higher than the currently recommended doses may be more efficacious (24). There are also reports that suggest that a higher dose of RMP is efficacious without serious adverse effects (25, 26, 27). A number of previous studies showed that low serum levels of INH and/or RMP could be problematic because they are associated with low therapeutic efficacy and relatively high therapeutic failure (28, 29, 30). Although limited data are available on dose and toxicity, physicians may be concerned that attempts to increase the dose of anti-TB drugs may lead to an increase in the frequency of anti-TB DIH. However, in the present study, we demonstrated that the serum levels of anti-TB drugs are not related to DIH development. The serum levels of first-line anti-TB drugs were normal in most of the patients, regardless of the presence of hepatotoxicity. The findings obtained after the inclusion of patients with mild LFT result elevation were also quite similar. Meanwhile, unlike the concentrations of INH or other drugs, the metabolic ratio of plasma acetyl-INH to INH levels 2 hr after drug ingestion was significantly lower (P<0.001). in the hepatotoxicity group than in the non-hepatotoxicity group in the present study. This result suggests that the serum slow acetylator status of INH may be a risk factor for anti-TB DIH. However, INH was presumed to be the causative drug in only 2 patients among the 12 patients in the hepatotoxicity group. To date, the influence of acetylation rate on INH hepatotoxicity is controversial (6). Nevertheless, INH is generally known to be one of the major causes of DIH in the treatment of TB, and is metabolized to hepatotoxic intermediates mainly by N-acetyltransferase (NAT). Reports linking polymorphic NAT acetylator status with DIH have been published and have indicated that slow acetylators are a risk factor for anti-TB DIH and that patients are prone to developing more severe hepatotoxicity than with rapid acetylators (9, 21, 31). Although the pathogenesis of INH-induced hepatotoxicity is not fully ascertained, our study suggests that the dose or serum concentration of INH resulting from INH metabolism may in part play a role in DIH by INH or another anti-TB drug.
Our study has several limitations. This study was limited by its retrospective nature. Serum drug level was not determined at the time of hepatotoxicity, which may have provided more information about DIH. Basal serum drug level may not be directly associated with anti-TB DIH. Furthermore, serum anti-TB drug levels may not always represent those of the target organ, such as the lung or bronchus. Pharmacokinetic variability would be observed for RMP and INH, although many pharmacokinetic and pharmacodynamic studies revealed usual serum time to peak concentration of INH, RMP, PZA is 2 hr (7, 29, 32). The literature review did not reveal any prospective correlation between plasma drug levels of anti-TB drugs and DIH. The maximum concentration (Cmax; mg/L) or Area under the concentration (AUC) curve might be a better predictor of DIH than peak serum drug levels. According to one recent prospective study, Cmax among 0, 1, 2, and 4 hr (mg/L) and AUC curve from 0 to 4 hr of INH and PZA were not different from DIH patients and controls but RMP level at day 7 could predict subsequent development of DIH in 93.3% of the patients (8). Another limitation of this study was the lack of specific information on the NAT genotype. If acetylator status was determined by genotyping, this addition information about the risk factor would have provided more definite results. However, the N-acetylator level could be determined indirectly through the metabolite level, which was also analyzed by TDM in the present study. Lastly, dose-related toxicity is not the only possible cause of DIH; idiosyncratic reactions, oxidative stress, or hypersensitivity to anti-TB drugs may also lead to DIH in some cases (22, 23). More research using TDM is needed to evaluate the TB drug plasma concentration and hepatotoxicity response relationship.
In conclusion, basal serum drug concentration is not associated with the risk of mild LFT abnormality or anti-TB DIH in patients being treated with the currently recommended doses of first-line anti-TB treatment drugs.

 XML Download
XML Download