

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of lower urinary tract symptoms (LUTS) in men increases with advancing age and LUTS represent one of the most common clinical problems in adult men (1). That tendency seems to increase continuously due to worldwide increased life expectancy. LUTS have a comparable negative impact on mental health and health-related quality of life as diabetes, cancer or hypertension (234). LUTS are associated with high medical and socio-economical costs and become burden on the healthcare system due to its rapid increase of prevalence in modern aging society (5). Therefore, research for finding LUTS-causing risk factors and the efforts to detect LUTS early in men with those risk factors is necessary. Traditionally, LUTS have been believed to be caused by prostate-related pathologies such as benign prostatic enlargement. However, many recent studies have shown that LUTS have complex multifactorial etiology (6). Even though voiding and storage symptoms often coexist, the mechanism is known to be different like detrusor overactivity during storage phase and underactivity during voiding phase (7).
Depressive disorder is also a very common and serious medical problem especially in older adults. Depressive disorder was ranked as 11th global burden of disease among the 291 diseases and injuries in 1990-2010 (8). In Korea, the prevalence of depressive disorder including major depressive disorder and dysthymic disorder in the 2011 national survey was 7.5% for the population aged 18-74 yr increasing with industrialization (9). Depression is a major mental illness that can cause functional disability (10), decreased quality of life, and excess mortality (11). Depression is also a risk factor for various chronic diseases such as chronic obstructive pulmonary disease (12), hypertension (13) and diabetes (14).
Because LUTS and depression have multifactorial etiologies and impact on various medical conditions, functional disability, and quality of life, close association between LUTS and depression is expected. Although some studies have investigated their association, most of them had various limitations resulting from small sample size (1516171819), incomplete LUTS assessment (15), inadequate covariates adjustment (17) and selection bias (1619). Most importantly, although prostate volume (PV) is one of the important predictors of LUTS (20) and the candidate confounder in the association analysis between depression and LUTS, none of them had considered it. We recruited 10,275 generally healthy 30 to 79 yr old men from a large health screening cohort, which included lifestyle factors, anthropometric variables, and most known LUTS-associated clinical variables such as PV data. We checked whether depression and its severity are associated with total, storage, and voiding symptoms.
MATERIALS AND METHODS
Study population
Eligible subjects were 30 to 79 yr old Korean men who underwent routine comprehensive health check-up from November 2007 to July 2013 at the Healthcare System Gangnam Center of Seoul National University Hospital. All subjects were requested to complete a structured self-questionnaire to collect information about depressive symptoms, LUTS status, current medical conditions, medications, alcohol consumption and smoking. Among 10,392 subjects, we excluded those with history of prostate cancer (n=23), those taking medications for LUTS (n=84), and those who received surgical treatment for prostate related problems (n=10), leaving 10,275 subjects. Anthropometric measurement and blood test were done at overnight fasting state.
Lower urinary tract symptoms and depression
International prostate symptom score (IPSS) was used to assess the severity of LUTS. The IPSS is composed of 7 questions ranging from 0 to 5 points each so that the total scores can be in 0-35 range (21). Severity of LUTS was classified as none to mild (0-7), moderate (8-19), or severe (20-35) using standard cut-off of IPSS. We further classified subjects into moderate to severe voiding symptoms (5 or more out of 20 points for weak stream, straining, incomplete bladder emptying, and intermittency) and moderate to severe storage symptoms (4 or more out of 15 points for urinary urgency, urinary frequency, and nocturia) (22).
Depression state was assessed using Beck Depression Inventory-II (BDI-II) questionnaire revised in 1996, a self-reported validated screening instrument for depression (23). The BDI-II contains 21 items that involve somatic and cognitive-affective dimension so that the total score can be ranged from 0 to 63. Depressive state was classified into 4 groups of none (0-13), mild (14-19), moderate (20-28) and severe (29-63) according to BDI-II criteria.
Assessment of LUTS-related clinical risk factors
Age was stratified into 10-yr age intervals, i.e. 30-39, 40-49, 50-59, 60-69, and 70-79. Smoking status was reported as one of three categories: never, former, and current smoker. Participants were asked to report the frequency and amount of alcohol consumption. Alcohol consumption amount was defined as never, under or equal to 4 drinks and greater than 4 drinks, where a standard drink means 14 g of pure alcohol (24). Weight and height were checked by the same automatic device and weight in kilograms was divided by the square of height in meters (kg/m2) to calculate body mass index (BMI). Participants were defined as hypertensive when subjects were taking antihypertensive medication or systolic blood pressure was ≥140 mmHg or diastolic blood pressure was ≥90 mmHg. Subjects were defined as having diabetes mellitus when subjects were taking oral hypoglycemic agents or insulin injection or HbA1c level was ≥6.5% or fasting glucose level was ≥126 mg/dL. Prostate volume (PV) was measured in milliliter using transrectal ultrasonography (TRUS) by a radiology specialist in those who voluntarily wanted PV test (n=1,925).
Statistical analysis
Comparison of demographic, depression status, lifestyle, and clinical features between subjects with none to mild LUTS and moderate to severe LUTS were performed by two-tailed Student's t-test for continuous variables and chi-square test for categorical variables. The variables associated with LUTS at a P value of less than 0.20 were included for further evaluation. A backward stepwise regression model to exclude variables showing associations with LUTS at a P value of more than 0.05 was used. Finally, the relative contribution and additional dose-response association between depression severity and LUTS status were estimated using a multivariate logistic regression analysis. A trend test for a linear trend of the log odds was used to assess P for trend across ordered depression categories. We also performed same multivariate logistic regression analysis by storage and voiding symptoms subcategories. In addition, to see the independent effect of depression on LUTS irrespective of PV state, multivariate logistic regression analysis after adjustment for PV status was also performed in subjects with PV data. All statistical analyses were performed using Stata version 13.1 (Stata Corp, College Station, TX, USA). All quantitative data are presented as the mean±standard deviation (SD) unless otherwise noted.
RESULTS
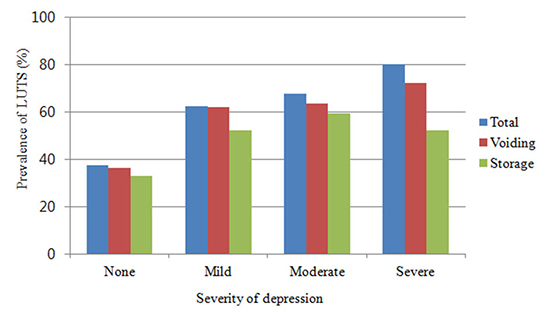
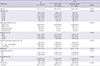
General characteristics of 10,275 study subjects are presented in Table 1. The prevalence of depression and LUTS were 5.8% and 39.1%, respectively. Subjects with LUTS were more aged, depressive, hypertensive, diabetic, and showed more alcohol consumption amount, lower BMI, and larger PV in univariate analysis. Additionally, we evaluated general characteristics between subjects who took TRUS and subjects who did not take TRUS (Supplement Table 1). There are significant differences of age (P<0.001) and LUTS state (P<0.001). Subjects who took TRUS are more aged and showed more severe LUTS (total, voiding and storage) in univariate analysis. Whereas there are no significant differences of depression state (P=0.215) in univariate analysis. We assume that as people become aged and suffer from LUTS, they worry about their prostate-related health problem such as prostate cancer and hyperplasia. Therefore, when they decide to take comprehensive health check-ups, they tend to include prostate-related tests like TRUS. To estimate relative contribution of depression and its severity for LUTS, we performed multivariate logistic regression as described in the methods. The logistic model included depression severity, age, smoking status, alcohol consumption amount, BMI, hypertension, and diabetes mellitus (Table 2). Compared to men without depression, mild, moderate, and severe depression were strongly associated with total LUTS (adjusted odds ratio [aOR], 2.99, 3.86, and 8.99, respectively: all P<0.001). Increasing severity of depression was significantly associated with an increasing trend of LUTS (P for trend<0.001). Some studies have suggested that a different cut-off value of BDI would be appropriate to Korean population because Koreans tend to have higher average of BDI than other countries (25). Thus we additionally performed the same logistic analysis according to the suggested Korean BDI score criteria and found similar results (Supplement Table 2).
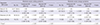
We also performed the same logistic analysis to evaluate the associations between depression severity and both voiding and storage symptoms (Table 3). Compared to men without depression, mild, moderate, and severe depression were associated with significantly higher voiding symptoms prevalence (aOR, 3.04, 3.28, and 5.58; all P<0.001). The same significant associations were also observed in storage symptoms (aOR, 2.43, 3.43, and 2.89; P<0.001, P<0.001 and P=0.011, respectively). Furthermore, increasing severity of depression was also associated with increasing trends of voiding and storage symptoms (all P<0.001).
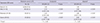
We additionally evaluated the effect of depression and its severity on LUTS independently of PV status by adjusting PV state for 1,925 subjects with PV data (Table 4). Mild depression was significantly associated with total, voiding, and storage symptoms (aOR, 3.29, 2.73, and 2.63, respectively; all P<0.001), however, only moderate-to-severe depression was significantly associated with total LUTS (aOR, 2.84; P=0.018). In case of voiding and storage symptoms, a tendency toward significant association was shown albeit with insufficient statistical power, most likely due to small sample size in this subgroup (aOR, 2.11 and 2.00; P=0.065 and 0.074, respectively).
DISCUSSION
Our study demonstrated that depression and its severity are strongly associated with total LUTS, voiding, and storage symptoms independently of PV status. Most importantly, we showed subjects with more severe depression have greater probability of LUTS.
Several previous studies have demonstrated a positive relationship between depression and LUTS (1516171819). However, they have many limitations which made their findings difficult to be generalized. Johnson et al. (17) reported that patients with depression had 156% higher American Urological Association Symptom Index scores than patients without depression. However, they adjusted only socioeconomic confounding factors (i.e. education level and income) besides age, not considering other LUTS-causing clinical factors. Based on the data from 2005-2006 and 2007-2008 NHANES, a cross-sectional study was conducted in 2,890 men (15). It reported significant relationship between LUTS and depression/suicidal ideation. However, LUTS assessment was made by using only 3 questions for nocturia, without taking into account emptying and hesitancy, and the severity for the 3 symptoms were not evaluated. Chung et al. (16) conducted a short-term prospective study for 2,000 Chinese men older than 65 yr and reported increased risk of depression in subjects with moderate to severe LUTS. However, this study only included elderly aged ≥65 yr and did not include any medically measured data such as blood test. Most importantly, all the previous studies had not included PV state in their model.
Although these studies reported consistent positive association between depression and LUTS, the biological mechanism behind the reported significant association between depression and LUTS remains unclear. Even though well designed longitudinal study need to be done to clarify the causal relationship, we believe that epidemiological and biological evidences are more favoring the causal effect of depression on LUTS.
In aspects of epidemiology, the prevalence of LUTS in men older than 70 yr is known to be about 40% mainly by effects of prostate hyperplasia while that in women older than 70 yr is relatively very low including in Korea (26). If we assume that LUTS is one of major causes of depression, the prevalence of depression in men is expected to be significantly higher than that in women. However the prevalence of depression is actually higher in women (9.1%) than men (4.3%) (9). Therefore, we think that there is a strong possibility that depression is the cause of LUTS rather than LUTS is the cause of depression.
The most likely hypothesis in biological aspects is dysregulation of corticotropin-releasing hormone/hypothalamic-pituitary-adrenal (CRH/HPA) axis in depression unlike normal stress response (27). Hypersecretion of CRH leads to sustained hypercortisolism and excessive activation of sympathetic nervous system that can cause many physical adverse effects. Persistent activated sympathetic nervous system also can make LUTS more severe, especially voiding symptoms rather than storage symptoms by affecting urethral smooth muscle through sympathetic innervation.
Serotonin (5-HT) is generally reduced in depression and deficiency of serotonin promote depressed state (27). Steers suggested that decrement of 5-HT in the central nervous system may predispose people to depression and overactive bladder (28). In an animal study, administration of 5-HT receptor agonists had effect that decrease the bladder activity and increase the activity of external urethral sphincter (29).
On the other hand, psychological as well as physiological factors may influence the relationship between depression and LUTS. Depressed patients tend to report worse symptoms than their actual state subjectively due to pessimistic perception. Considering that our results showed significant association between depression and LUTS independently of PV, which is important biological factor of LUTS, psychological factors may partly explain this relationship besides physiological factors.
Our study has many strengths compared to the others. Firstly, we included a large study population over 10,000 subjects encompassing nearly all adult age group contrary to previous studies which usually included less than 1,000 participants in specific age group. Secondly, we assessed depression and LUTS severity using validated structured questionnaire. Thirdly, we included nearly all known LUTS-related risk factors using lifestyle, anthropometric, and laboratory information. Most importantly, we included PV status for analyis which is one of the most important predictor of LUTS and can play a role as a key confounding factor in the association analysis between depression and LUTS.
Our study also has a few limitations. First, due to our study being cross-sectional in design, we were not able to specifically investigate the causality between depression and LUTS. Second, we did not have information about anti-depressant medication. However, most Koreans are reluctant to take anti-depressant medication, so its proportion in the study sample would be negligible (30). Furthermore, subjects taking anti-depressants are more likely to be classified into lower depression categories due to medication effects, which may have weakened our positive effect sizes due to its higher LUTS prevalence. Therefore, if we were able to properly classify subjects taking anti-depressants, our results likely would have shown higher degree of positive association between depression and LUTS.
In conclusion, depression and its severity are strongly associated with total, voiding, and storage symptoms independently of PV. It may be beneficial to evaluate for LUTS status in patients with depression. Longitudinal studies with more PV data across various ethnicities are needed to clarify the causal relationship.

 XML Download
XML Download