

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity can cause hypertension, hyperlipidemia, and cardiovascular disease (1). In Korea, with the recent westernization of lifestyles, the prevalence of obesity is gradually increasing (2).
There are 2 primary ways to evaluate obesity: body fat percentage (BF%) and body mass index (BMI, kg/m2). Body composition (i.e., the specific determination of body fat distinct from lean tissues such as bone and muscle) is theoretically better for evaluating excess adiposity than BMI. However, many techniques for measuring body composition in vivo are not feasible or inaccurate in epidemiological research settings (3). Therefore, BF% is not considered the gold standard for determining obesity whereas BMI is considered the gold standard for determining obesity.
In 1993, a World Health Organization (WHO) Expert Committee proposed BMI cut-offs of 25.0-29.9 kg/m2 and ≥30.0 kg/m2 for overweight and obesity, respectively, which have been used as the gold standard; meanwhile, in 2000, the Western Pacific Regional Office (WPRO) of WHO recommended cut-offs of ≥23 kg/m2 and ≥25 kg/m2, respectively, in the Asia-Pacific region (4). However, in 2004, a WHO expert consultation addressed the debate about the interpretation of these recommendations for Asian populations and determined that population-specific BMI cut-off points are not necessary. Lowering cutoff values by three units (as seems appropriate for Hong Kong Chinese, Indonesians, and Singaporeans) would have been too much for other populations (e.g., northern Chinese and Japanese). Where the indicated change in BMI cut-off values would be small (e.g., from 30 kg/m2 to 29 kg/m2), the wisdom of making a change for such a minor difference in weight could be questioned (3). Furthermore, the association between BMI and BF% depends on age and sex and differs between ethnic groups (5). Currently, the accuracy of BMI for detecting adiposity in the Korean population is unknown.
Therefore, this study aimed at assessing the diagnostic performance of BMI using WPRO of WHO reference standards for BF% (6), which define obesity as BF% ≥25% and ≥35% in men and women, respectively. In addition, we aimed at determining the optimal BMI cut-off for BF%-defined obesity for adults in Korea and comparing these results to those from a Western population to determine the appropriate difference in BMI values.
MATERIALS AND METHODS
Data source and study subjects
The data for this study were obtained from the Third Korean National Health and Nutrition Examination Survey (KNHANES III), which was a cross-sectional and nationally representative sample survey conducted by the Korea Centers for Disease Control and Prevention from 2007 to 2009. The survey was performed using stratified multi-stage clustered probability sampling to select a representative sample of the non-institutionalized civilian Korean population, resulting in 12,722 individuals in 4,000 households who were sampled. Of these, 10,533 individuals participated in the surveys (overall participation rate, 82.8%). Participants aged 20-69 yr (n=6,685) were included. Those individuals with incomplete anthropometric measurement data such as height, body weight, or dual-energy X-ray absorptiometry (DXA) were excluded (n=668), resulting in 6,017 subjects (2,623 men and 3,394 women) who were included in the final statistical analysis.
Study measurements
The survey consisted of a health interview survey that was conducted via face-to-face interviews in the participants' homes and a health examination survey via direct standardized physical examinations conducted in specially equipped mobile examination centers. The sequence of the health survey included intake, informed consent, anthropometric measurements, and completion of the questionnaire.
Anthropometric data, including height and body weight, were measured according to standardized guidelines. Standing height (cm) was measured using a mobile stadiometer (SECA 225®, SECA Deutschland, Hamburg, Germany) with the head and hip touching the wall. Body weight (kg) was measured using a mobile scale (GL-6000-20®, CASKOREA, Seoul, Korea) while the patient was dressed in a light gown without shoes. BMI was calculated as body weight (kg) divided by the square of height (m) (kg/m2).
Body composition was assessed, in light clothing without shoes or jewelry, by DXA (QDR 4500A®, Hologic Inc., Bedford, MA, USA) equipment located in the mobile examination centers. The results of the DXA were analyzed using industry standard techniques and the Korean Society of Osteoporosis with Hologic Discovery software (version 13.1) in its default configuration. The equipment was calibrated daily with the phantom supplied by the manufacturer. Whole body BF% (fat mass/total mass × 100) and lean mass (kg) were analyzed.
Definition of obesity
To determine obesity, we used the cut-off points recommended by the WPRO of WHO , as mentioned above (≥23 kg/m2 and ≥ 25 kg/m2 for overweight and obesity, respectively) (4). For BF%, we used the WHO standard definitions for obesity: ≥25% in men and ≥35% in women. Accordingly, the subjects were divided into normal and obese BF% groups (6).
Statistical analysis
The data were analyzed following the Analytic and Reporting Guidelines. Continuous and categorical variables are presented as mean±standard deviation (SD) and as frequencies, respectively. The diagnostic performance of BMI for detecting obesity defined according to BF% using the standardized cut-off points was calculated by receiver operating characteristic (ROC) curve analysis. The sensitivity, specificity, and positive and negative predictive values were calculated by sex and age (by decade). In addition, the optimal BMI cut-off for BF%-defined obesity was determined by constructing receiver operating characteristic curves.
RESULTS
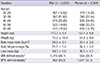
The analysis included 6,017 subjects, 2,623 men (49%) and 3,394 women (51%), for whom the weighted mean BMIs were 24.2± 3.1 kg/m2 and 23.4±3.5 kg/m2, respectively. The mean BF% values in men and women were 21.5%±5.2% and 32.3%±5.2%, respectively. According to the WPRO of WHO definition of obesity, 38.7% of men and 28.1% of women were classified as obese. Meanwhile, 25.2% of men and 31.1% of women were classified as obese according to BF% (Table 1).
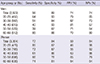
Regarding the diagnostic accuracy of BMI for detecting BF%-defined obesity, a BMI cut-off ≥25 kg/m2 had a high specificity (89%, men; 84%, women) but poor sensitivity (56%, men; 72%, women). The diagnostic performance of BMI decreased with increasing age, except in men in their 60s (Table 2).
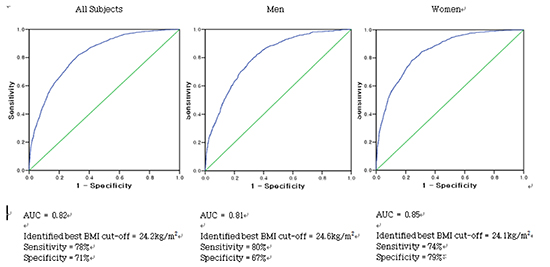
Fig. 1 shows the ROC curves for detecting BF%-defined obesity using BMI as well as the diagnostic performance for the optimal BMI cut-off in all subjects and by sex. Overall, the area under the curve was 0.82 for BMI to detect excess BF%, and the optimal cut-off was 24.2 kg/m2, which resulted in 78% sensitivity and 71% specificity; after stratifying by sex, the optimal cut-offs for men and women were 24.6 kg/m2 (80% sensitivity and 67% specificity) and 24.1 kg/m2 (74% sensitivity and 79% specificity), respectively.
DISCUSSION
In the present study, obesity was identified in 38.7% of men and 28.1% of women using body mass index (≥25 kg/m2) and in 25.2% of men and 31.1% of women using body fat percentage. A body mass index cut-off ≥25 kg/m2 had high specificity (89%, men; 84%, women) but poor sensitivity (56%, men; 72%, women).
BMI cut-offs are used to screen high-risk individuals, identify individuals for absolute risk assessment, select the type and intensity of treatment, monitor the temporal effects of treatment, determine institutional policies for individuals, and increase individuals' awareness of personal risks (3). It should be kept in mind that BMI is merely weight, adjusted for height. Moreover, the relationships between BMI and fat-free mass and body composition are limited (7).
In the present study, a BMI cut-off ≥25 kg/m2 had poor sensitivity (56% in men; 72% in women) for detecting BF%-defined obesity, especially when compared to that in the USA for the same cut-off (84%, men; 88%, women). However, the sensitivity in both populations at a cut-off of ≥25 kg/m2 was better than that for ≥30 kg/m2 in the USA (36% in men; 49% in women) (7). In the present sample, BMI also showed limited accuracy for diagnosing adiposity in specific groups according to age and sex, such as men in their 40s and 50s.
A recent large cohort study involving East Asian populations, including Koreans, revealed that the risks of cardiovascular disease and death are lowest in subjects with BMIs of 23-27 kg/m2 (8). Meanwhile, another study reported lower risks for BMIs of 21.5-27.9 kg/m2 (9). Furthermore, the 2004 WHO expert consultation did not recommend using population-specific BMI cut-offs for obesity (3). Despite the recommendations and recent evidence, the WPRO of WHO BMI standards are still officially used in Korea.
A comparison of the prevalence of obesity by country using large-scale NHANES data would help to determine if population-specific cut-offs are needed. In the present study using data from the KNHANES III (2009), 38.7% of men and 28.1% of women were classified as obese according to the WPRO of WHO cut-offs. Meanwhile, in the USA NHANES (2009) (10), 35.5% of men and 33.4% of women were classified as obese according to the global WHO BMI cut-off ≥30 kg/m2. It is unexpected that the prevalence of obesity is higher in Korean men than in American men. Therefore, obesity in Korea may be overdiagnosed owing to an inappropriately low WPRO of WHO BMI reference standard. This finding is also consistent with the WHO expert consultation recommendation in 2004 (3) that the global WHO BMI cut-off points should be retained as international classifications. Because the BMI cut-off point for observed risk in different Asian populations varies from 22 kg/m2 to 25 kg/m2; for high risk it varies from 26 kg/m2 to 31 kg/m2, the cut-off points of 23, 27.5, 32.5, and 37.5 kg/m2 are to be added as points for public health action.
On the basis of BF%, 25.2% of men and 31.1% of women were classified as obese in the present study compared to 50% of men and 62% of women in American populations (10). Thus, BF% better reflects the current status than population-specific cut-off points for BMI for international comparisons of the prevalence of obesity. The prevalence of BF%-defined obesity was higher in women than in men in Korea, which suggests that Korean women have less lean mass than do Korean men.
If the BMI cut-off for obesity in Korea (≥25 kg/m2) is likely too low, it would be useful to determine what the BMI in Korea should be, in comparison with that in other countries, to determine excess fat. In the present study, the BMI cut-offs for BF%-defined obesity in both sexes combined, men, and women were 24.2 kg/m2 (sensitivity, 78%; specificity, 71%), 24.6 kg/m2 (sensitivity, 80%; specificity, 67%), and 24.1 kg/m2 (sensitivity, 74%; specificity, 79%), respectively; in the USA (8), the respective cut-offs are 25.5 kg/m2 (sensitivity, 83%; specificity, 76%), 25.8 kg/m2 (sensitivity, 78%; specificity, 70%), and 25.8 kg/m2 (sensitivity, 85%; specificity, 88%). Therefore, the difference in BMI cut-offs for detecting BF% between Koreans and Americans is approximately -1.2 in both sexes and men and -1.0 in women. These differences are smaller than the 5-unit difference in BMI cut-off values between the WPRO and the global WHO obesity criteria. Therefore, the present findings support the address by the 2004 WHO expert group that small differences in cut-offs are questionable and population-specific BMI cut-off points are unnecessary (3).
The major strengths of this study are that national statistics from the KNHANES III were used and body fat composition was measured by DXA. The DXA technique has been validated for the measurement of fat-free mass and fat mass and used a standard test in many previous studies (11). However, differences in calibration between DXA technique instruments produced by different manufacturers, as well as between different models produced by the same manufacturer, have been reported. DXA (QDR 4500A®, Hologic Inc., Bedford, MA, USA) tended to underestimate fat mass (12). DXA had limitations of the weight of the scanning bed (typically 136 kg) and the width of the scanning area (usually ~60 cm), so it might contribute to underestimate the prevalence of BF%-defined obesity (13).
A limitation of this study is that only cross-national comparisons of the optimal BMI cut-offs for BF%-defined obesity were performed to determine what the BMI cut-off for the Korean population should be. Further, the clinical significance of BF% and its population-specific standard are not yet clearly defined.
Another limitation of this study is that direct comparison between two studies is difficult. Bioelectrical impedence analyzer (BIA) was used to estimate BF% in the USA instead of DXA in our study. However according to one study in Korean obese women, the correlations and agreements between estimates of BIA and DXA were highly significant (11).
Additional studies are required to define appropriate differences in BMI cut-offs between Asia-Pacific populations and the rest of the world. In addition, as most epidemiological studies involve BMI, future studies on morbidity and mortality should define obesity according to BF%.
In conclusion, BMI showed limited accuracy for diagnosing adiposity by age and sex in Korea. The difference between the optimal BMI cut-off for BF%-defined obesity in Korea and that in America was approximately -1.3 kg/m2. This difference is smaller than the 5-unit difference in the BMI cut-off value between the WPRO and global WHO obesity criteria.

 XML Download
XML Download