

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiovascular disease (CVD) is the major cause of morbidity and mortality in patients with diabetes. Dyslipidemia, a common condition coexisting with type 2 diabetes, is a major cause of atherosclerosis and a risk factor for CVD. Numerous studies have shown that lowering lipid levels is very important for preventing CVD in patients with diabetes (12).
Since their release, the guidelines of the Third Adult Treatment Panel (ATP-III) of the National Cholesterol Education Program have been used globally in the treatment of hyperlipidemia (34). The ATP-III guidelines defined patients with diabetes as coronary heart disease equivalent condition and high risk of CVD group. Individuals at high risk with low-density lipoprotein cholesterol (LDL-C) levels ≥ 100 mg/dL are candidates for statin therapy. The ATP-III guidelines calculated the 10-yr risk of coronary heart disease (CHD) using the Framingham risk calculator (5).
The American College of Cardiology and the American Heart Association (ACC/AHA) guidelines for the management of cholesterol were released in November 2013 (6). The new guidelines expand the recommendation for statin therapy to all patients with diabetes aged 40-75 yr with LDL-C levels ≥ 70 mg/dL who also have a 10-yr risk of CVD ≥ 7.5%, as estimated based on new pooled cohort equations (7).
In Korea, the prevalence rate of dyslipidemia increased from 1998 to 2010, but the treatment rate of diabetic patients in 2010 was only 23.6% (8). This study used data from the Korea National Health and Nutrition Examination Surveys (KNHANES) to estimate the number of patients with diabetes in Korea for whom statin therapy would be recommended based on the new guidelines compared with the ATP-III guidelines.
MATERIALS AND METHODS
Study population
This study was performed using data from the KNHANES V (2010-2012) conducted by the Division of Health and Nutritional Survey under the Korean Centers for Disease Control and Prevention (KCDCP). This is a nationwide, community-based cross-sectional survey examining the general health and nutrition status of the civilians of Korea. Participants were selected from sampling units based on geographical area, sex, and age group using household registries and a stratified, multistage, clustered, probability sampling design. This sampling method is certified to produce representative statistics by the Korea National Statistical Office.
The diagnostic criteria for diabetes were taken from the American Diabetes Association (ADA) guidelines (9). Patients over 30 yr of age were defined as having diabetes if they had already been diagnosed as diabetic by a physician or had a fasting plasma glucose level ≥126 mg/dL or HbA1c level ≥6.5%. We excluded participants who fasted less than 8 hr before blood sampling and who had missing LDL-C level data. After these exclusions, a total of 1,975 patients with diabetes for whom LDL-C levels that were directly measured or calculated by Friedewald's equation were available (10).
The diabetic patients were divided into dyslipidemia treatment versus non-treatment groups. The patients in the dyslipidemia treatment group were defined as those who reported taking medications for dyslipidemia. Treatment for dyslipidemia was not limited to statins but included any type of drug. We assessed the eligibility for statin therapy using the 2004 updated ATP-III criteria as well as the 2013 ACC/AHA guidelines. According to the ATP-III guidelines, patients with diabetes should be considered at high risk. Statin therapy is recommended in high-risk patients with a LDL-C level ≥100 mg/dL. The new ACC/AHA guidelines recommend moderate-intensity statin therapy in all diabetic patients between the ages of 40 and 75 yr and moderate-to-high-intensity statin therapy in those with a 10-yr risk of CVD ≥7.5%.
Biochemical measurements
After fasting for 8 hr or more, blood samples were drawn from the antecubital vein of each participant in the morning. Samples were processed appropriately, refrigerated at 2-8℃, and transported to the Central Testing Institute, Seoul, Korea. After transport, plasma was separated by centrifugation and analyzed within 24 hr.
The fasting plasma concentrations of glucose and lipid were measured using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). High-performance liquid chromatography (HLC-723G7; Tosoh, Tokyo, Japan) was used to measure HbA1c.
The HDL-C level was calculated according to the Lipid Standardization Program of the US Centers for Disease Control and Prevention (CDC). The formula used in 2012 was different from that in 2010-2011. LDL-C levels have been measured directly using automated enzymatic techniques since 2009 in KNHANES IV. LDL-C levels were calculated using Friedewald's formula (11) in subjects with no direct LDL data.
Statistical analysis
All statistical analyses in this study were performed using weighted variables with stratification and clustering variables to incorporate sample weights and to adjust for the complex sample design of the survey. Nominal variables are presented as the numbers of cases and percentages, and continuous variables are presented as means±standard deviations. We compared the baseline characteristics of men and women by Student's t-test and chi-square test. We determined the proportion of the patients with diabetes in KNHANES for whom statin therapy would be recommended on the basis of the two guidelines.
We calculated the new ACC/AHA pooled-cohort equations to determine the proportions of adults with a 10-yr risk of CVD ≥7.5%. All analyses were conducted using SPSS version 19.0 software (IBM, Chicago, IL, USA).
RESULTS
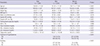
A total of 25,534 individuals participated in the health interview and examination in KNHANES V in 2010-2012. Of these, 17,292 subjects were ≥30 yr of age, among whom 12.5% (2,165 patients) had diabetes. A total of 190 participants was excluded because of missing LDL-C data, leaving 1,975 patients (aged 62.64±11.42 yr, 30-90 yr) with diabetes analyzed in this study. Table 1 shows a comparison of the baseline characteristics between men and women. There was no difference in HbA1c levels between men and women (7.3 vs. 7.3, respectively, P=0.996). Women were older than men (64.11 vs. 61.24, respectively, P<0.001) and had higher levels of total cholesterol and LDL-C (193.2 vs. 182.61, respectively, P<0.001; 115.61 vs. 108.65, respectively, P<0.001). A larger proportion of female patients (23.9%) than male patients (14.5%) had been taking medications for dyslipidemia.
Fig. 1 shows the flow of the process used to determine the final subjects selected for analysis according to the two sets of guidelines for the management of cholesterol. Among the 1,598 diabetic patients who had never taken medications for dyslipidemia, 1,048 patients (65.6%) were recommended for statin therapy according to the NCEP/ATP-III guidelines. According to the new ACC/AHA guidelines, 94.3% (72.8% required moderate-to-high-intensity therapy; 21.5% required moderate-intensity therapy) were recommended for statin therapy.
Among the 1,975 Korean adult diabetic patients, 19.1% (n=377) had already been taking drugs for dyslipidemia. If patients with LDL levels >130 mg/dL were recommended for statin therapy, an additional 25.3% (n=500) would be classified as requiring statin therapy. After application of the NCEP/ATP-III guidelines, an additional 53.1% (n=1,048) were classified as requiring statin therapy. Application of the new ACC/AHA guidelines resulted in an indication for statin therapy in an additional 76.2% of patients (n=1,506) (Fig. 2).
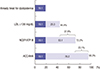
Among the 1,598 patients not taking any drugs for dyslipidemia, according to the NCEP/ATP-III guidelines, more female patients and those aged <60 yr required statin treatment than did male patients and those aged ≥60 aged (69.7% vs. 62%, respectively; 68.7% vs. 63.6%, respectively). On the other hand, according to the ACC/AHA guidelines, more patients required statin treatment among males and those aged ≥60 yr than did females and patients aged <60 yr (94.5% vs. 93.8%, respectively; and 97% vs. 89.9%, respectively) (Fig. 3).
DISCUSSION
Over the past two decades, many randomized controlled trials have shown that lowering LDL-C levels with statin therapy reduces the incidence of atherosclerotic CVD under clinical conditions (1213). The new ACC/AHA cholesterol guidelines were developed based on this evidence and emphasize primary prevention of cardiovascular disease. In diabetic patients, the new guidelines suggest that most patients require statin therapy. The 2015 ADA guidelines accept this concept of statin therapy for primary prevention in diabetic patients (14). We estimated the percentage of Korean adult diabetic patients requiring statin therapy according to the two sets of guidelines using the KNHANES data.
In this study, female Korean diabetic patients had higher levels of total cholesterol and LDL-C despite the larger portion taking drugs for dyslipidemia. As the mean age of women was older than that of men, it is possible that the group of women included a larger number of those older than 50 yr. According to a previous study, in the Korean general population, men had more hypercholesterolemia and hyper-LDL-cholesterolemia among the younger aged population (<50 yr), whereas among those of older age (≥50 yr), women had more hypercholesterolemia and hyper-LDL-cholesterolemia. Women had higher HDL-C levels in all age groups (8). The same difference in HDL-C level was also found in American national data (1516). In this study, Korean diabetic patients showed no differences in HDL levels between men and women. This may have been because diabetic patient have low levels of HDL-C.
We estimate that under the new guidelines, 94.3% of diabetic patients will be indicated for statin therapy, representing almost all patients with diabetes. This population would represent an increase of 28.7% over the number currently eligible according to the ATP-III guidelines (65.6%). These new treatment recommendations have a larger effect in older aged (≥60 yr) than younger aged individuals (<60 yr) and in men than women (Fig. 3). These trends are similar to those in the general population in the USA (17). The differences according to age may be partially explained by the new pooled-cohort equations (7). The new equation targeted prevention of stroke and coronary heart disease, as the prevalence of CVD rises markedly with age (18). In the Korean population, approximately 90% of old people require statins for primary prevention according to the new guidelines (19). However, there are few data showing the benefit of statin treatment in older people without CVD (20). Instead, younger individuals were shown to require more aggressive preventive treatment for CVD. The new guidelines would also result in more men being newly indicated for statin therapy than women, although women had worse dyslipidemia. This may be explained by the new guidelines also expanding the indication for statin therapy among adults with other risk factors for CVD, even at lower levels of LDL-C. More male than female patients are smokers.
The purpose of treatment of dyslipidemia is not simply normalization of cholesterol level itself, but also the prevention of CVD and a decrease in mortality rate. Diabetes is a serious risk factor for CVD. Therefore, the ADA recommended statin therapy for all patients with diabetes aged >40 yr without additional CVD risk factors, with consideration of moderate-intensity statins for primary prevention (14). However, it remains unclear whether Asian diabetic patients should follow these guidelines. The Japan Atherosclerosis Society (JAS) recommends a goal of LDL-C level <120 mg/dL for the high-risk group as well as diabetes for primary prevention (21). These recommendations are based on Japanese epidemiological studies (222324). These studies indicated that low-dose statins are effective for prevention of atherosclerotic CVD (ASCVD) in Japanese patients. Several studies showed that relatively low-dose statins had a high lipid-lowering effect in Korean subjects (252627). According to the new guidelines, high-intensity statins are a taken at a daily dose that lowers LDL-C by an average of approximately ≥50%, e.g., atorvastatin 40-80 mg or rosuvastatin 20-40 mg. Moderate-intensity statins are taken at a daily dose that lowers LDL-C by 30%-50%, such as atorvastatin 10-20 mg or rosuvastatin 5-10 mg. A clinical study in Korea showed that atorvastatin at 10 mg decreased LDL-C levels by 41.8% from baseline, and a decrease of 48.8% was observed with only 5 mg rosuvastatin. In another Korean study, there were no differences in major adverse cardiac events between high-intensity and low-to-moderate-intensity statin therapy in patients with acute myocardial infarction (26). Therefore, it may be possible for Korea to reach the same goal of CVD prevention as the new guidelines but with relatively lower doses of statin. However, it is still controversial as to which statins and doses are most effective, as the Korean absolute CVD risk is lower than those in Western countries, and there are insufficient long-term data. Even among Asian ethnic differences in cardiovascular mortality (28), respective countries need their own guidelines for prevention of ASCVD.
Nevertheless, Korean diabetic patients have not received appropriate management for dyslipidemia. We showed that only 19.1% of diabetic patients were taking antidyslipidemic medications. As these medications include any drugs for dyslipidemia, the real proportion of patients taking statin may be smaller than 19%. If we assume the goal is to lower LDL-C levels to <130 mg/dL, an additional 25.3% of patients need statin therapy. This level is higher than the JAS guidelines for diabetic patients. Even according to the ATP-III guidelines, an additional 53.1% of patients require statin treatment. At present, the Korean national health insurance system guarantees statin therapy in cases with LDL-C levels >100 mg/dL. Therefore, more than half of all diabetic patients in Korea have not received statin therapy. It is necessary to at least ensure that diabetic patients are managed according to the proper guidelines.
This is the first study regarding application of the new cholesterol guidelines to Korean diabetic patients. We used validated national data from KNHANES V (2010-2012). However, we did not consider peripheral vascular disease or previous cardiovascular events and did not predict real effects of the new and old guidelines on diabetic patients due to a lack of Korean cohort data.
In conclusion, the new ACC/AHA guidelines would increase the indication for statin therapy of most diabetic patients. The issues involved with application of the new guidelines to the Korean diabetic population should be discussed further in future studies. At present, many diabetic patients do not receive appropriate statin therapy. Efforts should be made to ensure that more diabetic patients receive appropriate statin therapy and to develop the Korean guidelines.


 XML Download
XML Download