

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a systemic inflammatory disease of unknown cause. RA patients have higher all-cause mortality compared to general population of the same age and gender without RA. The most common cause of death is due to accelerated atherosclerosis, especially coronary artery disease; the incidence of myocardial infarction is 30%-60% higher (1), and its onset is approximately 10 yr earlier in RA (23). The age- and sex-adjusted mortality rate from cardiovascular disease (CVD) in RA patients is 50%-100% higher than that in the general population (4). Increased prevalence of diabetes, hypertension, hypercholesterolemia, and metabolic syndrome in RA can explain the higher mortality, however, RA itself is also responsible for the excess of cardiovascular morbidity and mortality (5). The traditional atherosclerotic risk factors alone cannot explain the accelerated atherosclerosis in RA patients. Some studies have reported that chronic inflammation might play a major role in accelerated atherosclerosis (6). Inflammation can cause not only abnormal lipid metabolism, but also transformation of fatty streak to unstable plaque. In addition, there is growing evidence that atherosclerosis is an inflammatory disease (7).
Regarding the CVD risk, Framingham risk score (FRS), the 10-yr risk of CVD in age between 20 and 79, can be used - scoring age, smoking history, systolic blood pressure, total cholesterol, high density lipoprotein, and fasting glucose according to sex (8). Atherosclerosis is a chronic disease that remains asymptomatic for decades, and complicates CVD such as stroke or heart attack. Flow mediated dilation (FMD), pulse wave velocity (PWV), augmentation index (AIx), central blood pressure, and carotid intima media thickness (CIMT) are available as non-invasive measurements for evaluation of atherosclerosis (9). CIMT is one of the most widely used non-invasive tests of atherosclerosis, and employed by clinicians and clinical investigators to assess the risk of cardiovascular disease. The carotid artery is a good candidate for study using high-resolution ultrasound devices because it is located superficially, relatively stationary, and runs parallel to the surface of the neck at least to the level of the carotid bifurcation. In 1986, Pignoli et al. reported CIMT as a non-invasive method for measurement of atherosclerosis (10), and a strong predictor of future vascular events. In asymptomatic persons older than 45 yr, CIMT measurement can add incremental information to the traditional risk factor assessment for primary prevention. Furthermore, increases in CIMT were directly associated with the risk of stroke and coronary artery diseases such as acute myocardial infarction (AMI) in older adults (11).
Regarding increased prevalence of coronary artery disease and high CVD mortality rate, chronic systemic inflammation and enhanced instability of atherosclerotic plaques are suggested as other factors in RA in addition to the traditional CVD risk factors (12). RA patients treated with disease-modifying anti-rheumatic drugs (DMARDs) showed a reduced risk for CVD compared to those without DMARDs (13). Suissa et al. reported on a case control study that RA patients with any DMARDs showed decreased prevalence of AMI (14). The purpose of this study was to evaluate the effects of RA and anti-rheumatic drugs on atherosclerosis by comparing CIMT as an indicator of the risk of CVD in RA patients.
MATERIALS AND METHODS
Procurement of subjects
This study was designed as a case-control study. With informed consent, age-, sex-matched control subjects and RA patients were recruited evenly according to age group. Of patients diagnosed as RA at the Yeungnam University Hospital, a total of 44 female patients from each age group were included in this study (5 RA patients aged ≤40 yr; 17 of 41-50 yr; 15 of 51-60 yr; 7 of ≥61 yr). All the patients met the 2010 ACR/EULAR criteria for RA (15). Of persons who consented to routine medical examinations and CIMT measurement at the Yeungnam University Hospital Health Promotion Center, 22 age-matched healthy females (2 aged ≤40 yr; 10 of 41-50 yr; 8 of 51-60 yr; 2 of ≥61 yr) without abnormal laboratory findings or past medical history were enrolled as control subjects. Those with a body mass index (BMI) >25 kg/m2, hypertension, history of smoking, cardiovascular diseases; coronary artery disease, heart failure, symptomatic carotid artery disease (CAD), peripheral artery disease, abdominal aortic aneurysm, diabetes, malignancy, active infection, other metabolic disorders, and currently taking lipid lowing drugs were excluded from this study.
Evaluation of subjects and measurement of CIMT
Blood pressure was measured twice using an electrical sphygmomanometer. BMI was determined as the individual's body mass in kilogram divided by the square of their height in meter. Persons with normal blood pressure in the range from 120 over 80 (120/80 mmHg) to 140 over 90 (140/90 mmHg), and BMI within normal ranges (18.5 kg/m2 ≤BMI ≤25 kg/m2, respectively) were included in this study. Serum C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), white blood cell, platelet counts, hemoglobin, total cholesterol, high dense lipoprotein (HDL), triglyceride (TG), and low density lipoprotein (LDL) levels were tested. CIMT was measured on both carotid arteries using a B-mode ultrasound (Medison, Korea™ EKO7, 12 MHz linear transducer, Samsung Medison Co., Seoul, Korea). Images were obtained on the views parallel to the common carotid artery from the claviculo-sternal junction to the carotid bifurcation. Double echo pattern representing the combined width of the intima-media complex could be readily and reproducibly visualized in all subjects. At three different points on each side where a double-line pattern is observed without plaque, CIMTs were measured, and the mean value of both sides was taken as the CIMT of the subject.
Assessment of RA disease activity
For assessment of RA activity, disease activity score 28 (DAS 28) was determined. A rheumatologist evaluated 28 joints for swelling and tenderness in RA patients. The 28 joints examined were, both metacarpo-phalangeal joints, both second to fifth proximal interphalangeal joints, both first interphalangeal joints, both elbow, both shoulder and both knee joints. With the counts of tender and swollen joints, ESR and the patient's subjective assessment (SA) score, DAS 28 was calculated using the following numeric formula.

TEN28, tender joint counts 28;
SW28, swollen joint counts;
ESR, erythrocyte sedimentation rate (mm/hr);
SA, subjective assessment of disease activity during the preceding 7 days on a scale between 0 and 100
In RA patients, the uses of steroids, non-steroidal anti-inflammatory drugs (NSAIDs), and DMARDs were assessed as well as the traditional CVD risk factors. Accumulated dose of steroids was calculated equivalently to that of prednisolone. Hydroxychloroquine (HCQ), leflunomide (LFM), and MTX were included as DMARDs, and CIMT was evaluated in RA patients according to the CVD risk factors, disease activity and the use of anti-rheumatic drugs.
Statistical analysis
Statistical analysis was performed using SPSS version 18. Paired t-test, Student t-test, two-way ANOVA for parametric analysis and Wilcoxon singled rank test, Mann-Whitney test, Wilcoxon signed rank test, Spearman's rank correlation test and Friedman test were used for non-parametric analysis. Analysis of correlation between the determinants was performed using Spearman's rho test and adjusted using multivariate regression tests. Distribution of all parameters was checked by Kolmogorov-Smirnov test. The values were statistically significant with a confidence interval of 95% and a P value<0.05.
RESULTS
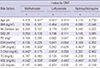
As the CVD risk factors, age, the levels of BMI and cholesterol showed no difference between healthy control subjects and RA patients. However, CIMT in RA patients was significantly thicker than that of healthy control subjects (0.705±0.198 mm, 0.611±0.093 mm, respectively, P<0.05). Significantly higher levels of ESR and serum CRP were observed in RA patients compared to those in healthy control subjects (26.93±23.46 mm/hr, 16.14±8.18 mm/hr, respectively, for ESR, P<0.01; 0.71±2.09 mg/dL, 0.05±0.05 mg/dL, respectively, for CRP, P<0.05) (Table 1).
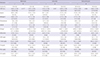
With adjustment for the conventional CVD risk factors, the effects of RA and anti-rheumatic drugs on atherosclerosis were analyzed by comparison of CIMT between RA patients and healthy control subjects. Adequate control of inflammation and disease activity is the target of treatment in RA. Glucocorticoids (GC), NSAIDs and DMARDs are used to attain low disease activity or remission. The accumulated dose of GC was calculated as the sum of the equivalent dose of prednisolone. Blood total cholesterol, TG, HDL-, LDL-cholesterol levels, disease duration, BMI, DAS 28 and CIMT did not differ significantly between the subgroups according to the use of GC. Age and ESR level were higher in RA patients treated with GC, as compared to those in RA patients without GC (61.08±8.48 yr, 55.0±11.90 yr for age, respectively, P<0.05; 28.39±25.04 mm/hr, 20.38±13.64 mm/hr for ESR, respectively, P<0.01). Blood total cholesterol, TG, HDL-, LDL-cholesterol levels, disease duration, DAS 28 and CIMT were not different between the subgroups by the use of NSAIDs. Higher BMI was observed in RA subgroups with NSAIDs than in RA without NSAIDs (23.02±3.24, 20.23±1.84, P<0.05, respectively) (Table 2).
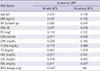
The most commonly used DMARDs in RA patients were MTX, LFM, HCQ, and sulfasalazine (SSZ). The DMARDs were used either singly or in combination (Table 3). In a dummy-variable regression analysis, among the DMARDs, a decrease of CIMT was observed only in RA patients using MTX (P<0.01). The GC dose, DAS28, and disease duration did not differ between the age-, sex-matched RA subgroups with or without MTX. CIMT in RA without MTX was thicker than that with MTX (0.767±0.233 mm, 0.644±0.136 mm, respectively, P<0.05) even with significantly lower levels of total cholesterol, LDL cholesterol, HDL cholesterol, and BMI. CIMT in RA showed no difference according to the use of LFM. However, higher ESR, BMI, GC dose, and LDL cholesterol level were observed in RA patients with LFM than in those without LFM. No difference in CIMT was observed in RA according to the use of HCQ either, even with significantly lower total cholesterol and LDL cholesterol levels in RA with HCQ. CIMT of RA patients and RA patients without MTX was thicker than that of healthy control subjects. However, in RA patients treated with MTX, CIMT did not differ from that of healthy control subjects. In contrast to MTX, the use of LFM or HCQ yielded no effect on CIMT in RA patients. The current study showed that among the DMARDs, MTX may exert favorable effects on CIMT independently to the disease activity of RA (Table 4).
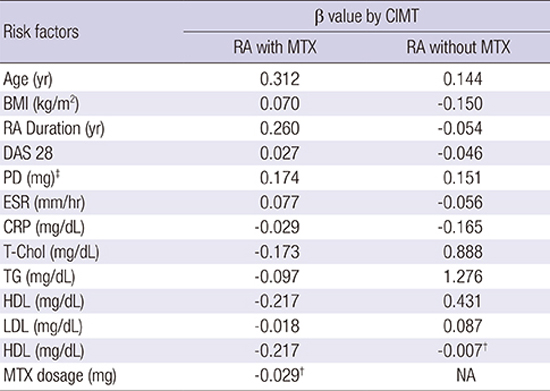
Additionally, in analyses of CIMT according to the clinical factors and the use of DMARDs in RA, a correlation between CIMT and age was observed in RA without MTX (r=0.338, P<0.05), but not in RA with MTX (Table 5). In a multivariate regression analysis among the drugs, the use of MTX showed significant correlation with CIMT (β=-0.177, P<0.05). When adjusted for the conventional CVD risk factors, age, disease duration, DAS28, total GC dose, ESR and CRP levels, the maintenance dose of MTX in RA patients showed significant negative correlation with CIMT. For each 1 mg increase in MTX dose, there was a 0.029 mm decrease in CIMT (P<0.01) (Table 6).
DISCUSSION
In RA patients, thicker CIMT and more frequent plaques of the carotid artery are observed (16); and the findings are correlated with the degree of articular damage (17). Coronary artery atherosclerosis detected as calcification was more severe and more prevalent in patients with established RA than in patients with early disease and control subjects (1819). Ten-year cardiovascular mortality could be predicted in the group of patients with rheumatoid factor (RF)-positive inflammatory arthritis once the baseline CRP was elevated (20). The current study showed a higher CIMT in RA patients as compared to healthy subjects of the same age, sex, BMI, and cholesterol levels without history of smoking or hypertension.
Steroids can be associated with atherosclerosis, which can damage the vessel wall, and then increase the cardiovascular disease morbidity (2122). Blood pressure can be elevated. And disturbance of glucose and lipid metabolism, hypercoagulability, platelet activation and endothelial cell damage can occur in subjects taking steroids. Davis et al. reported that RF-positive RA patients were at increased risk of CV events, particularly with higher cumulative exposure, higher average daily dosage (>7.5 mg/day), and recent use of GC (23). Wei et al. reported that patients with DMARDs and high dose steroid had higher risk of CVD in inflammatory arthritis (24). In addition to the steroids, excessive risk of CVD has been reported for some NSAIDs (2526). Lindhardsen et al. reported an association of NSAID exposure with a 22% increase in risk of cardiovascular events among RA patients; and this was significantly lower than the NSAID-associated risk increase (51%) observed in control subjects (27). On the contrary, a small beneficial effect of NSAIDs on the risk of cardiovascular mortality was also reported in a cohort of inflammatory polyarthritis patients (25). In this study, the use and accumulated dose of GC and NSAIDs had no effect on CIMT in RA. The effects of GC and NSAIDs on CIMT of RA in the current study may be a consequence of shared inflammatory mechanisms between RA and atherosclerosis.
Suissa et al. reported an association of the use of DMARDs with a decreased rate of myocardial infarction (14). However, Solomon et al. reported a higher risk for CV events in patients who had received cyclosporine, azathioprine, or LFM (22). Use of MTX in RA patients showed an association with a reduced risk of CV events compared to RA patients without MTX (28). Some studies suggested possible mechanisms of MTX on atheroprotection by modulating AMP-activated protein kinase - cyclic AMP response element-binding protein (AMPK-CREB) pathway in intramural MTX therapy to prevent neointimal thickening following angioplasty (29), and in chronic systemic inflammation of murine model (30). Reiss et al. reported an athero-protective effect on MTX on a cell model. MTX promotes reverse cholesterol transport via activation of adenosine A2A receptor, and limits foam cell formation in THP-1 macrophages (31). In one report, atherogenic lipid profiles of RA patients improved after specific therapy for arthritis (32). However, no relationship of mortality was observed with the use of SSZ, HCQ, penicillamine, and intramuscular gold.
The current study evaluated the effects of DMARDs on atherosclerosis in RA patients. A favorable effect of MTX on CIMT was observed. As adjusted for the conventional risk factors and clinical factors, the use and the maintenance dose of MTX had atheroprotective effect on CIMT that was not consistent with LFM, HCQ or SSZ in RA. The mechanisms for this possible benefit may be that MTX can reduce the disease activity and systemic inflammation and progression of atherosclerosis. However, the use of DMARDs for RA with an efficacy similar to that of MTX was not associated with decreased CVD mortality (33). In this study, even with the same age, disease activity and inflammation levels lower CIMT was observed only in the patients using MTX. Therefore, it is suggestive that MTX may have direct protective effects to atherosclerosis in addition to the anti-inflammatory effects.
This study has some limitations as a case-control study in a small numbered population. Exclusion of participants with CAD or aneurysm to avoid influences of treatments, dividing RA patients into drug related small groups and manual measurement of CIMT are the main limitations. A large numbered, randomized-controlled, prospective study measuring CIMT by a software is required.
Early diagnosis and treatment of RA have been emphasized to prevent radiologic progression of joints. However, in this study, the authors verified an athero-protective effect of MTX on CIMT in addition to the effect on arthritis. Measurement of CIMT for atherosclerosis may be important not only to clarify the CVD risk but also to evaluate the effectiveness of treatment in RA. And, the use of MTX should be considered in high priority not only to control arthritis but also to suppress atherosclerosis and RA-related CVD risk to mortality.
 XML Download
XML Download