

 PDF
PDF ePub
ePub Citation
Citation Print
Print



CONCEPT AND DELIVERY OF CRITICAL CARE
Critical (or intensive) care medicine (CCM) is a branch of medicine concerned with the care of patients with potentially reversible life-threatening conditions. Patients often present with, or are at least at risk of, multi-system illnesses. CCM therefore requires sophisticated diagnoses, multiple organ support, and invasive monitoring. As CCM deals essentially with patients who have a reasonable chance of recovery, it should be distinguished from other disciplines dealing with serious irreversible medical conditions such as advanced cancer. CCM also differs from emergency medicine because it provides a continuum of care from initial resuscitation to recovery to home.
For optimal critical care, a multidisciplinary team is essential and includes 1) medical and nursing directors with authority and co-responsibility for intensive care unit (ICU) management; 2) collaboration between nursing, respiratory therapy, and pharmacy staff and medical staff in a team approach; 3) use of standards, protocols, and guidelines to assure a consistent approach to medical, nursing, and technical issues; 4) dedication to coordination and communication for all aspects of ICU management; and 5) emphasis on practitioner certification, research, education, ethical issues, and patient advocacy (12).
The physician or the intensivist involved in CCM should be qualified because CCM requires a thorough understanding of pathophysiology and is centered initially on the resuscitation of patients at the extremes of physiologic deterioration.
ROLE OF THE INTENSIVIST AND ICU DEVELOPMENT IN KOREA
The Korean Society of Critical Care Medicine (KSCCM) defines intensivists as follows: physicians who are board certified in a medical specialty as acknowledged by the Ministry of Health and Welfare, who received education, training and subspecialty board certification specifically in critical care in designated qualified institutions by the KSCCM, and who work closely with other experts to provide their patients with ongoing and consistent care.
Numerous studies have been conducted to investigate the effects of the presence of an intensivist on clinical outcomes and cost-effectiveness. In a systematic review, ICUs with an intensivist showed the relative risk of death to be 0.42-0.85 of that of ICUs without an intensivist (3). In Korea, ICUs with an intensivist have a lower mortality than ICUs without an intensivist in the case of patients with severe sepsis/septic shock (4). In another study performed during the H1N1 influenza epidemic, ICUs with an intensivist showed a lower mortality than ICUs without an intensivist (5).
Many studies also demonstrated favorable cost-effectiveness of intensivist (678). In these studies, the intensivist resulted in shorter ICU stays, decreased use of resources, and lower re-admission rates.
Since the early 2000s, KSCCM has put an enormous amount of effort into persuading the Ministry of Health and Welfare and also the medical professional group about the need for intensivists. On the 12th January 2010, a public hearing was held at the National Assembly, where the KSCCM asserted the need for intensivists in ICUs to opinion leaders of legislation, major media, policy makers (the Ministry of Health and Welfare, the Health Insurance Review and Assessment Service), citizen representatives (Green Consumer Network in Korea). In 2008, through these efforts, CCM was acknowledged as a subspecialty of medicine by the Korean Academy of Medical Sciences.
To educate potential intensivists, the KSCCM has a training and qualification committee. The requisites to participate in the board examination include 1 yr of training at an accredited institution, attendance of both a basic critical care review course (BCCRC) and a multidisciplinary critical care review course (MCCRC), which are endorsed by and run in collaboration with the Society of Critical Care Medicine of the USA. Certification should be renewed every 5 yr, and requires ongoing medical education equivalent to at least 100 points (1 hr of education is 1 point, not exceeding 6 points per day of education). Intensivist training is available only at institutions accredited by the training and examination committee. The accreditation is renewed every 3 yr after a rigorous audit. The requirements for accreditation include the institution should 1) be tertiary hospital or secondary hospital with at least two relevant specialties, 2) fulfill the facilities and equipments as dictated by law, 3) have 2 or more critical care subspecialists involved in education, 4) have documents for education programs.
STATUS OF KOREAN ICUs: ORGANIZATION, CHARACTERISTICS OF PATIENTS, NURSE AND PHYSICIAN STAFFING (2009 vs. 2014)
In 2009, critical care specialists in charge of all 136 critical care training hospitals nationwide completed a questionnaire survey. Among the ICUs, 56.4% were located in or near the capital city. Only 38 ICUs (17.3%) had intensive care specialists with a 5-day work week. The average daytime nurse-to-patient ratio was 1:2.7. Elderly people ≥65 yr of age comprised 53% of the adult patients. The most common reasons for admission to adult ICUs were respiratory insufficiency and postoperative management. Staffing was worse in areas outside the capital city (9).
In 2009, there were a total of 975 ICUs and 10,446 ICU beds in Korea, according to data released by the National Health Insurance Corporation. The estimated 17 adult ICU beds per 100,000 population is comparable to that in other advanced countries (10). Besides medical infrastructure, we are confident that medical science and technology in South Korea has grown to a level nearly equal to that in advanced countries. However, we cannot say that the management and outcomes in critical care units have reached the same levels as those in advanced countries. It is clear that there are substantial differences between countries with respect to clinical performance, medical resources, and national spending on healthcare. Nevertheless, our findings and their implications raise some serious issues, which may account for the poor outcomes.
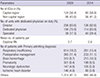
A follow-up nationwide survey on ICUs was performed in 2014. Critical care specialists in charge of all 136 critical care specialty training hospitals nationwide responded to the questionnaire. According to an interim analysis, 58.8% of the ICUs were located in or near to the capital city (Table 1). Only 40 ICUs (29.4%) had intensive care specialists with a 5-day work week. The average daytime nurse-to-patient ratio was 1:2.6. Elderly people ≥65 yr of age comprised 50% of the adult patients. The most common reasons for admission to adult ICUs were respiratory insufficiency and postoperative management.
In 2014, there were a total of 838 ICUs and 10,165 ICU beds in Korea, according to data from the National Health Insurance Corporation. The interim results in 2014 survey were similar to those of the 2009 survey.
In the Table 1 are also described the organization and staffing of ICUs in Korean universities and teaching hospitals, as well as the characteristics of admitted patients (2009 vs. 2014). The data collected in this survey indicate that nurse and physician staffing is poor compared with that in advanced countries. We believe that the roles of healthcare professionals are important, and considerable effort, including enhanced reimbursement of critical care costs, must be made to improve the quality of critical care at the national level.
WHAT ISSUES SHOULD BE ADDRESSED FOR PROPER CRITICAL CARE IN KOREAN SOCIETY?
Compared with the status of critical care in other countries, there are many aspects of delivery of critical care that have to be addressed to establish a more vibrant system in Korea. First and foremost, the cost of reimbursement of critical care must be addressed. Although the level of reimbursement for in-patient care is generally low in Korea, this is especially true for patients cared for in ICUs. Hospital administrators are reluctant to invest in personnel and equipment in the ICU because of this. For example, although we have seven tiers of reimbursement for ICU room charges according to the number of nurses in the unit, the difference in room charges is not nearly sufficient to entice the hospital administrators to invest in better patient care by having more nurses per unit.
Another important problem is related with the definition of ICU as used by the Ministry of Health. According to the definition, presence of medical doctor is not mandatory to be classified as an ICU. Theoretically, a unit can be called an ICU with a nurse seeing 8-9 patients per shift without a doctor being present in the unit. It is well known that patients have better outcomes if there is an intensivist working in the ICU (14581112). The number of patients per nurse per shift is also an important determinant of outcome (141113). It is fortunate that the government has finally mandated that an intensivist be present in ICUs of tertiary centers starting this year. However, the regulations still do not specify that the doctor working as an intensivist be properly trained, and no upper limit has been set on the number of patients the doctor can properly manage simultaneously. Also, there is still no requirement for an intensivist in ICUs in hospitals that are not tertiary centers. In addition, critical care is truly a multidisciplinary endeavor that requires expert contributions from other specialists, including clinical pharmacists, nutritionists, and respiratory therapists (141516). In Korea, only a handful of hospitals receive daily support from these specialists, which may adversely affect outcomes.
Other problems also pose a threat to our critical care delivery system. There are huge differences in the level of care delivered at our hospitals. The mortality of patients cared for in ICUs during the 2009 H1N1 epidemic showed almost three fold differences in mortality (5). This may be due to the fact that not many ICUs have an intensivist. In a survey done by the KSCCM in 2009, only 17.3% of ICUs had full-time intensivists. As we discussed previously, the presence of an intensivist is one of the most important factors for improving quality of care. The low number of intensivists in Korean ICUs is particularly alarming because many of these patients are in an unstable condition and inter-hospital transport may adversely affect their outcomes. Thus, we need to develop good regional centers for critical care that can take care of patients in a particular region. The need for these regional centers was highlighted during the 2009 H1N1 influenza epidemic, when a lot of patients needed critical care and were too sick to be transported.
Lastly, the time has come for people working in ICUs to take interest in issues beyond direct medical care. Providing an environment where the patients can keep their dignity and receive psychological support is necessary (17). This is especially true for many patients already in an ICU who have had the goals of their care changed or need end-of-life care (18). Also, greater interest in the life of ICU survivors is needed to improve their physical and psychological well-being by decreasing post-ICU care syndrome (1920). This process should start with the realization that ICU care can leave a scar on ICU survivors and then proceed to providing support, including the administration of less sedatives and encouraging early mobilization (21).
If these concerns are not dealt with properly, it could have profound consequences. Globally, the cost of critical care is rising sharply with the increase in the elderly population (22). As Korea is one of the fastest aging societies in the world, it is imperative to plan for the sharp increase in demand for proper critical care. If we do not, there will be a shortage of intensivists, which will lead to poorer patient outcomes and further increases in the gap between hospitals with ICUs.
HOW TO PRIORITIZE THE CHANGES REQUIRED TO IMPROVE CRITICAL CARE
The low level of quality of critical care service in Korean hospitals necessitates system-level changes in the organization of critical care. A stepwise approach is needed to solve multifactorial failures in critical care delivery as described above. Time should be allotted to address difficult issues and solve barriers that urgently need attention to ensure better outcomes for patients in ICUs. Instead of investing money in upgrading hardware equipment in ICUs, investment should be directed toward implementing standardized ICU care under the supervision of a dedicated full-time critical care physician. This is the most urgent issue that needs to be addressed in our critical care system. A qualified full-time intensivist should be differentiated from a self-intensivist, who is only self-qualified for critical care. Secondly, an efficient critical care team should be developed and centered around a qualified full-time intensivist. The team does not need to be big at first, but it should be constituted so that communication is facilitated between members and it should have decision-making capability. The critical care team should strive to increase compliance with standardized care and reduce medical errors in ICUs. Also, it should monitor the implementation of essential measures in ICUs. The essential measures include a patient bedhead elevation of more than 30 degree, appropriate peptic ulcer prophylaxis and deep venous thrombosis prophylaxis, hand washing, appropriate antibiotic selection with respect to time and duration, catheter removal as soon as possible, effective assessment of pain and delirium, appropriate use of blood transfusions, and a low tidal volume strategy. Thirdly, relevant legal support should be improved. For this, a long-term task force consisting of all involved stakeholders including policy makers should be instigated. The task force should address critical care reimbursement, developing a legal standard for ICU organization that suits the level of the hospital, and surveillance for ICU quality improvement. Quality improvement should include outcome measures such as ICU mortality rate, length of stay, average days on mechanical ventilation, suboptimal management of pain, and patient/family satisfaction (23). Fourthly, a rapid response team (RRT) should be constituted at tertiary care hospitals. An RRT (commonly known as a medical emergency team) is distinct from a critical care team, which is confined to the ICU. Preemptive management of patients by RRTs is possible as long as the management is applied appropriately. Last, but not least, it is important to continually publicize what an ICU is to the general public and policy makers. While the concept of critical care has gained widespread acceptance among medical professionals and medical policy makers, the general public and even hospital administrators have lagged behind in recognizing the need for critical care, and the role of doctors specializing in it.
CONCLUSION
The goal of critical care is to reverse the acute, and sometimes life threatening, symptoms of patients with minimum sequelae in a cost effective and ethical way. This is a challenge that needs be addressed urgently in our healthcare system, because the need for appropriate ICUs has been increasing as our population rapidly approaches an aged society. A long-term task force consisting of all involved stakeholders should be implemented to address multifactorial barriers, such as unreasonableness in the critical care reimbursement system, shortage of critical care professionals, and the unacceptable level of the legal standard for the critical care delivery system. A capable critical care team with full-time intensivists is the first and most urgent requirement to improve care at ICUs. Intensivists should prioritize basic but essential management so that scarce resources are not exploited to the point of depletion. Publicity about ICUs to the general public is also urgently required to draw attention to the current suboptimal level of our critical care system.
 XML Download
XML Download