

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Conventional magnetic resonance (MR) imaging [e.g., contrast-enhanced T1-weighted (CE-T1) imaging with gadolinium and fluid attenuated inversion recovery imaging)] has been recommended for reliable delineation of intracranial tumors (12). However, because high-grade gliomas often diffusely infiltrate surrounding normal brain tissues, morphology-based target delineation using conventional MR imaging and computed tomography (CT) can miss lesions that should be included in the treatment volumes (345). Enlarging clinical target volumes (CTVs) to encompass suspicious regions which are not visible on CT and CE-T1 images of high-grade gliomas can hinder dose optimization for local high-risk regions. Moreover, image-based target definition including the tumor bed is even more critical for residual tumors after incomplete surgical resection to ensure coverage of the neoplastic regions and prevent recurrence (6). Thus, various attempts have been made to improve the radiation treatment outcome of high-grade gliomas by integrating multi-modal imaging, beam intensity-modulated techniques, and other adjuvant therapies (78910).
However, high-grade gliomas showed poor survival rates and frequent recurrence, even within the pre-irradiated gross tumor volume (GTV) receiving higher doses than marginal tumors (10). It CTV delineation considering physiological and histopathological characteristics of the tumor and dose optimization to high-risk regions that may be positively applied to create more effective treatment plans (11).
One of the characteristics for high-grade gliomas is increase of cellularity during tumor progression (12). Apparent diffusion coefficient (ADC) maps reconstructed from diffusion-weighted (DW) MR images can describe histopathological information about cellularity in high-grade gliomas (2), by providing a quantitative index of restricted water diffusion in intracellular spaces relative to extracellular spaces (13). Enhanced regions of malignant gliomas with compact cellularity on ADC maps (aCTVHR) can be used to define high-risk CTV (141516) and doses were optimized to the aCTVHR.
In this study, we defined aCTVHR on the ADC maps by making reference to the reported quantitative ADC criteria which indicates malignancy level of high-grade gliomas. The benefits of aCTVHR-targeted dose optimization were assessed in dose distributions of an intensity-modulated radiation therapy (IMRT) plan based on ADC values (IMRTADC) as compared with a conventional IMRT (IMRTconv) plan.
MATERIALS AND METHODS
Image acquisition
A patient was diagnosed with a high-grade glioma (grade III) in the right anterior temporal lobe and basal ganglia of the brain. After surgical resection of the tumor, ADC images of the cavity showed a suspicious malignant lesion; therefore, adjuvant radiation therapy was performed according to the National Comprehensive Cancer Network practice guidelines (17). To determine residual tumor volumes, we examined perfusion-weighted, MR spectroscopy, and DW images along with conventional MR and CT images.
MR imaging and CT were performed using a 1.5-Tesla MR unit (GE SIGNA system, GE Medical Systems, Milwaukee, WI, USA) and a GE 9800 Quick System CT scanner (GE Medical Systems), respectively. CE-T1 imaging used gadolinium as the contrast agent and a spin echo T1-weighted sequence with a time to echo (TE) value of 500 ms and a repetition time (TR) of 13 ms. The ADC maps were constructed from DW images that were scanned over 3 orthogonal diffusion gradients with 2 different gradient factors (b=0, 1,000 s/mm2) using a TE of 75 ms and a TR of 8,000 ms. To obtain reliable signal-to-ratio and consider clinically practical application of ADC maps, commonly applied b-value of 1,000 s/mm2 was used (18).
Incorporation of ADCs into the radiation treatment plan
ADC values were used to verify the severity of the residual malignant lesion and to differentiate the aCTVHR from the tumor bed. Average, maximum, and minimum ADC values and ADC ratios (rADCs) were calculated using MATLAB (version 7.10.0.499, MathWorks, Natick, MA, USA). To reduce variability in the selection of the boundaries of tumor regions, ADC values were evaluated in the compact rectangular volumes of interest (VOIs) covering all apices of the suspected regions closely surrounding hypo-intense voxels on ADC maps. Then, volumetric averaged ADC values were evaluated within the expanded VOIs (VOIs with at least a 2-cm margin on each side). Because high-grade gliomas often contain cystic or necrotic regions, we averaged the ADC values from 3-5 regions of interest (ROIs, 2-3 mm2 each) in the expanded VOIs. The rADC is obtained from the ADC of the aCTVHR divided by the ADC of the volume in contralateral normal brain tissues.
The aCTVHR showing a lower ADC value than the averaged ADC value was extracted via computational analysis and image processing of ADC maps. The extracted aCTVHR was re-marked on the ADC maps (pixel intensity equal to the maximum pixel intensity of the original ADC map). The ADC values were also confirmed by comparing with those reported for high-grade gliomas in diagnostic studies.
Because quantitative analysis of ADC maps and extraction of aCTVHR by applying the ADC criteria were not possible in commercial planning system (Eclipse, version 7.3.1, Varian Medical Systems, Palo Alto, CA, USA), two kinds of CT images were imported into Eclipse: the original CT images and another CT images including the aCTVHR and the CE-T1 image-based CTV (tCTV). To obtain the contours of the aCTVHR and tCTV on CT images using more reliable image registration functions, two sets of images (ADC map vs. CE-T1, CE-T1 vs. CT) were registered using BrainSCAN (version 5.31, BrainLab, Munich, Heimstetten, Germany). The overall procedure used to incorporate the determined aCTVHR into radiation treatment plans is shown in Fig. 1.
We also referred to the converted DW ratio to confirm volumes with low diffusion levels on DW-MR images. The DW-ratio maps were obtained by normalizing the original DW images to the average diffusion intensity of corresponding contralateral normal brain tissues.
Treatment plans
To evaluate dose distribution in the IMRTADC plan, the following tumor volumes were contoured on each CT image: CE-T1-based GTV (tGTV), ADC-based CTV (aCTVHR), and relative complement volume of aCTVHR in tCTV (sCTV) (Fig. 2).The tCTV is tGTV plus a 2.0-cm margin (1.5 cm for microscopic spread and 0.5 cm for set-up uncertainty). The CTV margin adjacent to critical structures, such as the right optic nerve, optic chiasm, and pituitary gland, was compromised to spare organs at risk (OARs).
The IMRTADC plan was optimized to deliver 60 Gy to the aCTVHR via the simultaneous integrated boost (SIB) technique (21719). Because the ADC maps indicated the differentiated
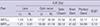
aCTVHR from the residual tumor, the tumor bed needed to receive the required dose of 50 Gy (16). However, because the IMRTconv plan was based only on conventional CE-T1 images, which showed the tumor bed but not CTVHR at the specific position, the tCTV received 60 Gy. The other plan parameters were equally applied to both plans, and they are summarized in Table 1. To provide a conformal dose to CTVs, 5 coplanar fields with different gantry angles (70°, 130°, 250°, 270°, and 310°) and 2 non-coplanar fields (60°/60° and 300°/300° for gantry/couch angles, respectively) were used.
Evaluation of dose distributions
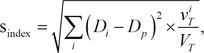
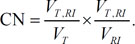
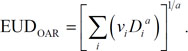
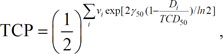
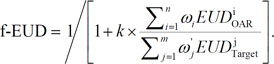
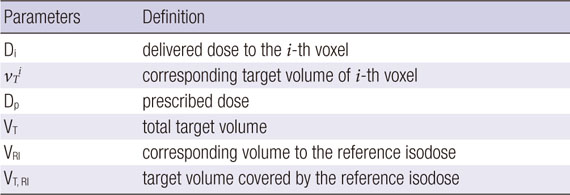
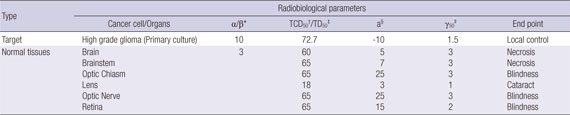
Dose distributions in the two plans were evaluated using biophysical indices for plan comparison and dose volume histograms (DVHs) for the aCTVHR and the tCTV. The homogeneity and conformity of dose distributions in the CTV were analyzed using the statistically modified homogeneity index (s-index) and the conformity number (CN), respectively (2021). The s-index and CN were evaluated using the prescribed doses (59.4 Gy for the aCTVHR and 50.4 Gy for the tCTV). Dosimetric effects were evaluated on the basis of the equivalent uniform dose (EUD) of the two plans according to a linear quadratic model for the tumor (2223) and a power law for the OARs (24). Tumor control probability (TCP) based on Poisson statistics was compared for the aCTVHR in both plans (25). In addition, the EUD-based figure-of-merit (f-EUD) was calculated for comprehensive plan evaluation using the EUD value of each primary structure (24). The weighting factors and the relative importance in f-EUD were assumed to be 1 in this study. Formulas and radiobiological parameters to evaluate dose distributions and calculate biophysical values are summarized in Appendix A and B (262728).
RESULTS
Clinical target volumes in multimodal images and apparent diffusion coefficients
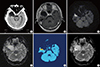
Conventional CT images did not clearly distinguish between the high-risk CTV and normal brain tissues (Fig. 3A). The resection cavity was enhanced by the contrast medium in the CE-T1 images (Fig. 3B), but the histopathological characteristics of the high-risk CTV were not apparent. In contrast, the DW images and ADC maps could reveal residual high-risk CTV as enhanced and suppressed regions, respectively (Fig. 3C, D). In the converted color map of the DW image, the diffusion values for the high-risk CTV were more than two-fold higher than those for normal brain tissues. Higher intensity regions appear red or orange in Fig. 3E.
The average ADC of the high-risk CTV was (0.73±0.23)×10-3 mm2/s, and the average rADC was (0.67±0.32)×10-3 mm2/s; both were less than 1×10-3 mm2/s. The minimum ADC of the high-risk CTV was 0.37×10-3 mm2/s, which is lower than the ADCs reported in medical diagnostic studies of high-grade gliomas [(0.86±0.12)×10-3 mm2/s and (0.82±0.13)×10-3 mm2/s for average ADC and rADC, respectively] (1529). The volumes with values lower than the average ADCs were defined as aCTVHR (Fig. 3F).
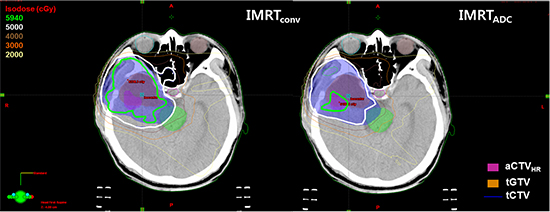
Plan evaluation
Dose distributions in two IMRT plans were evaluated using DVHs and various dosimetric metrics. The IMRTADC plan, which focused on dose optimization for the aCTVHR, produced a well-confined conformal dose distribution around the aCTVHR within the prescribed 60-Gy isodose surface (fluorescent green in Fig. 4A). Because dose conformity is mainly affected by the size of the total volume which received dose more than prescribed value (VRI) (area surrounded by fluorescent green line in Fig. 4B), the aCTVHR-targeted dose distribution resulted in less irradiation of the VRI. The IMRTADC plan improved the dose conformity of the aCTVHR up to 15 times, compared to the IMRTconv plan (Table 2). In addition, the IMRTADC plan showed superior dose uniformity of the aCTVHR by 7%, as indicated by a lower s-index in this plan compared with that of the IMRTconv plan.
Although the IMRTADC plan slightly increased the EUD (61.42 Gy vs. 60.00 Gy in the IMRTADC and IMRTconv plans, respectively) and the TCP (26.67 % vs. 24.01%, respectively), the differential DVHs of the aCTVHR were comparable in both plans (Fig. 5A). The DVHs showed greater dose sparing of OARs in the IMRTADC plan (Fig. 5B), owing to differences in dose optimization with and without focusing on the aCTVHR. The tailored dose delivery in the IMRTADC plan reduced EUDs by up to 16% in the brain stem and right lens (Table 3) and by more than 10% in the right optic nerve, optic chiasm, and left lens. Lower EUDs in these OARs could lead to an increase in f-EUDs in the IMRTADC plan.
DISCUSSION
Combining DW images and ADC maps with conventional CT and CE-T1 images can bring advantages in cancer diagnosis and therapy. In some cases, especially those involving high-grade gliomas with a rim that is not enhanced by contrast agents on CE-T1 images, DW images and ADC maps can help delineate CTVs by detecting pathologically relevant tumor characteristics not seen on conventional morphological images (5). As the large CTV is located close to critical organs, determination of image-based anisotropic target margin becomes more important for reducing toxicity in normal tissues. When we adopt DW images into radiotherapy plans for such as determination of target margins and high-risk CTV mentioned above, more rigorous image analysis and multimodality image-based confirmation of target volumes can support reliable application of advanced functional MR images.
Moreover, because DW images can show physiological and pathological variations of tumor to evaluate treatment responses through rapid and noninvasive scanning (30), those can be considered as an appropriate and powerful tool for adaptive radiation treatment plans. Patients can be monitored without additional radiation exposure during fractionated radiation treatment.
As application of extra-cranial DW images for patients with breast, prostate, and liver cancers (31) and the advent of a MRI-linac hybrid machine gradually become widespread, the role of DW images or ADC maps to define CTV becomes more important (32). Image-based dose optimization, especially targeting to the high-risk CTV, may facilitate effective and delicate dose delivery using dose painting techniques (33).
In conclusion, the aCTVHR was determined via quantitative analysis of ADC maps of a residual high-grade glioma. The IMRTADC plan in combination with DW images and ADC maps showed optimized dose distribution to the aCTVHR with dense cellularity. Incorporating ADC maps into radiation treatment plans for high-grade gliomas may help achieve biophysical dose optimization in local high-risk tumor volumes.





 XML Download
XML Download