

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Advance directives (ADs) document patients' wishes with respect to end-of-life care and who will make health care decisions for patients when they become incompetent (1). ADs allow patients to protect their autonomy and prevent their caregivers from having difficulty in making decision when patients are near death.
In Korea, so-called grand-mom Kim's Case has aroused public attention in protection of patients' autonomy, and has led to the efforts to reach an agreement regarding discontinuation of meaningless life-sustaining treatments (2). Sun et al. (3) reported that most terminal cancer patients in hospice centers had positive attitudes about the need of ADs. Although several hospitals have recently introduced ADs, ADs were not completed by patients but by their families in most cases (4). Because few patients have been given the right to decide end-of life care; to do or not to do (5, 6, 7), there has been a need of nationwide discussions on ADs.
In St. Vincent's Hospital, we have introduced an AD form for terminal cancer patients in the hospice center since October 2012 to enhance patient's participation on end-of life care decision. As one year has passed since the introduction of ADs, we aimed to analyze the current situation of ADs in real practice.
MATERIALS AND METHODS
We reviewed the medical charts for 214 terminal cancer patients who were admitted to the hospice center in St. Vincent's Hospital from October 2012 to September 2013. The AD form contained the following items: life-sustaining procedures, palliative sedation, and proxy selection. Life-sustaining procedures consist of cardiopulmonary resuscitation (mechanical ventilation, cardiac massage, electric cardioversion, extra-corporeal membrane oxygenation, and inotropics), high calorie artificial nutrition, and hemodialysis. The proxy is a surrogate decision maker assigned by patients in case they cannot make a health care decision on their own due to poor condition.
ADs were introduced to patients and their caregivers by a hospice coordinator on admission to the hospice center. After receiving consent from patient's caregivers for discussion of ADs with patients, a third-year resident who works on three-month shift explained the details of each item in the ADs to the patients. The patients specified whether they would receive or refuse each item and decided on a proxy.
The clinical characteristics were summarized as counts (percentage) for categorical variables, and as median values (range) for continuous variables. Comparison between patients who completed ADs and those who did not were analyzed using t-test for and chi-square test. The descriptive analysis was applied to preferences for life-sustaining treatments and the proxy. A P value<0.05 was considered statistically significant, and statistical analysis was performed using SPSS version 21.0.
RESULTS
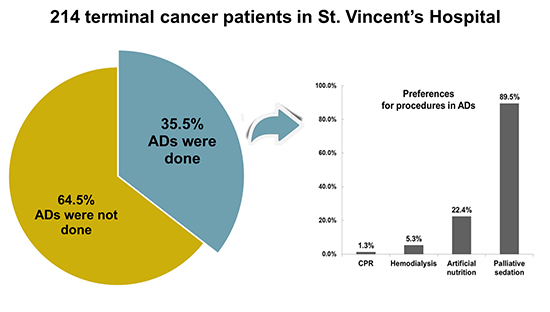
The median age of the patients was 67 yr (17-90) and 55.1% was male. The most common diagnosis was gastrointestinal cancer (33.2%) followed by lung cancer (26.6%). Most patients were educated (89.3%) and the majority had no religion (52.3%). Among 214 patients, 76 patients (35.5%) completed ADs on their own. Patients who completed ADs were younger (P<0.001), showed better performance (P=0.007), and had higher education (P=0.014) than patients who did not complete ADs (Table 1).
Of the 76 patients who signed ADs, 70 (92.1%) completed ADs with their caregivers. As for life-sustaining procedures, only one patient (1.3%) preferred cardiopulmonary resuscitation. Four patients (5.3%) wanted hemodialysis; of these, three had normal renal function, the remaining patient had third-stage chronic renal failure, and none of the patients received maintenance dialysis. Seventeen patients (22.4%) wanted artificial nutritional support; of these, seven had gastrointestinal cancer, four had lung cancer, four had hepatobiliary cancer, one had nasopharyngeal cancer, and one had peritoneal cancer. Sixty-eight patients (89.5%) wanted palliative sedation (Fig. 1). As a proxy, 55.3% preferred spouses, 28.9% sons/daughters, 7.9% siblings, and 6.6% parents (Table 2).
Ninety-seven patients (70.3%) did not complete ADs because their physical or mental condition was not sufficient to understand and make a decision regarding ADs. The other reasons were family's refusal to explain ADs to patients (2.9%), patient's refusal to complete ADs (3.6%), and unknown reasons (23.2%). Patients without ADs received end-of life care based on care level and discussion with family members. None of the patients received cardiopulmonary resuscitation.
Median time to complete ADs from admission was three (0-90) days, and the median duration of survival after completion of ADs was 22 (1-340) days. Patients who had completed ADs showed a significantly longer survival than those who did not: 27 (5-340) days and 16 (1-305) days, respectively (P=0.007).
DISCUSSION
In this study, approximately one third of patients completed ADs. Although this value is lower comparing with the existing research, it is meaningful that all ADs were completed by patients themselves. Kwon et al. (4) reported that 68% of patients in hospice centers had ADs completed, but only 4.8% were conducted by patients. The purpose of ADs is to reflect patients' self-determination and protect their autonomy. For this reason, patients' participation is most important. We briefly introduced ADs to patients and their caregivers on admission and obtained consent from caregivers for discussion of ADs with patients. After establishing rapport with patients, the doctor carefully explained ADs and helped them to complete ADs. It is believed that such a process could be helpful in making both patients and their caregivers understand the need for ADs, reducing their resistance to ADs, and involving more patients.
Few patients in this study wanted life-sustaining treatments. Yoon et al. (8) investigated cancer patients' acceptance of life-sustaining treatments in hospice centers, found that all of them refused cardiopulmonary resuscitation, intubation, and ventilator application, and 97.3% refused dialysis. It means that most terminal cancer patients did not want to receive any medical intervention that was invasive or just for the purpose of sustaining life. There was actually no case of cardiopulmonary resuscitation given in our hospice center during the period of the research. Patients wanted artificial nutrition more than life-sustaining methods or dialysis. Patients who wanted artificial nutrition included those having had no major problem with oral dietary intake as well as those for whom dietary intake was impossible due to gastrointestinal tumor or other conditions. This result is probably related to the cultural characteristics of Korea where nutrition is regarded as important.
Palliative sedation is administration of a sedative in order to decrease consciousness and relieve suffering when uncontrolled symptoms last. Palliative sedation was very highly preferred by patients in this study. No research has shown yet how many patients wanted or received palliative sedation in practice in Korea. Although the medical environment or cultural differences make it difficult to offer a direct comparison, research in Swiss patients who had completed ADs showed that 54% of them wanted palliative sedation for pain during the refractory period (9). Most patients in this study had insight of their terminal cancer on admission to the hospice center and the majority of them had pain or breathing problems; thus, there is a likelihood that they showed higher preference for palliative sedation since they were willing to spend the rest of their life without pain rather than to live longer. There is another likelihood that patients poorly understood what palliative sedation meant despite receiving a full explanation of it from their doctors.
As a proxy, the majority of patients in this study preferred their spouses. Research conducted among the general public residing in Seoul also showed that the majority (72.3%) gave the highest preference to their spouses as a proxy for end-of-life care (10). In contrast, Silveira et al. (11) found that sons/daughters or grandsons/granddaughters (60.3%) were most preferred, followed by spouses (29.6%), other relatives (7.6%), and unrelated ones (2.7%) in the United States. In Korea, people do not want to burden their son/daughters, which could be a possible reason for their preference for spouses as proxy.
Patients did not complete ADs because of their poor performance status due to their medical condition; because their families refused to have patients sign ADs; or because they themselves refused to sign ADs. Some of the reasons could not be determined through the review of medical charts, however possible reasons might be difficulty in facing patients with death through explaining ADs or the doctor's poor conversation skill. Since the doctors who recommend ADs to patients work on three-month shifts in this hospital, there are individual differences in understanding of the importance of ADs and in getting used to having conversations with patients about ADs. In order to have more ADs completed, patients should have access to ADs while they are in a better condition. A favorable attitude from both patients and their caregivers toward hospice-palliative care is also important (12). Doctors need to be skilled at having a conversation with both patients and their caregivers and to explain ADs positively to both of them on the basis of the emotional bond.
In this study, it took the patients a median of three days to complete ADs, and they died 22 days after signing ADs. Kwon et al. (4) reported that the median duration of survival after ADs were signed was nine days. In our study, ADs were completed relatively earlier; however, the duration of survival after the patients signed ADs is still very short.
This study has the following limitations. First, there were many cases in which the reason for not completing ADs was not found due to insufficient medical records. Second, we did not analyze whether the patients had actually received preferred medical interventions of ADs. Given that the physician is involved in the process of completing ADs, physician's order for life-sustaining treatment (POLST) seems to be a proper term. However, ADs and POLST were not used separately when we started ADs, and the term ADs is more widely used in similar studies. For this reason, we use the term ADs instead of POLST in this study.
In conclusion, one third of terminal cancer patients completed ADs on their own in the hospice center. Few wanted life-sustaining procedures, but palliative sedation was mostly accepted. Considering that patient's poor condition is the main reason for not completing ADs, earlier discussion regarding ADs while patients are in good condition is necessary in order to enhance patients' participation.


 XML Download
XML Download