

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative acute kidney injury (AKI) occurs frequently after coronary artery bypass surgery (CABG), worsening short-term and long-term clinical outcomes and survival, and increasing patient costs (123). Because there is currently no effective therapy for AKI, factors predictive of AKI and predictive models that estimate patient risk for AKI may be useful in optimizing perioperative care and preventing AKI in these patients. However, although several predictive risk models for AKI have been proposed, these models are currently limited by differing definitions, small cohorts, or a lack of validation (4).
Several recent studies suggested that elevated serum concentrations of uric acid may be associated with kidney disease without intrarenal uric acid crystal deposition (56). Additionally, hyperuricemia associates directly with hypertension, metabolic syndrome, chronic kidney disease, and peripheral vascular disease (7). Moreover, hyperuricemia is a common finding in patients with coronary vascular disease (78). Thus, preoperative hyperuricemia may be linked to an increased risk of AKI after CABG.
Recent few studies found a link between preoperative uric acid concentrations and postoperative AKI (91011), although these studies included the relatively small numbers of patients or several types of operations. Therefore, to confirm previous findings, we performed a retrospective cohort study investigating the association between preoperative elevated uric acid concentrations and the frequency of postoperative AKI in a large and homogeneous cohort of adult CABG patients. Furthermore, we also investigated whether preoperative uric acid is a useful predictor of postoperative AKI in patients undergoing CABG by discrimination and reclassification measures.
MATERIALS AND METHODS
A review of the Asan Medical Center Coronary Artery Bypass Surgery and Anesthesia Database identified patients who underwent CABG between January 1, 2006, and October 31, 2011. Information in this database was prospectively collected, beginning in 2006, for continuous assessment and improvements in quality of care for all patients undergoing CABG at our institution (12). Patients were excluded if their serum uric acid and creatinine concentrations were missing; if they had undergone preoperative dialysis; if they had undergone emergent surgery; if they had undergone any other type of cardiac surgery in addition to CABG; if they had a prior history of organ transplantation or nephrectomy; or if they had been treated with allopurinol. Patient data, including demographic, laboratory, and medication data, comorbidities, perioperative management, and mortality, were acquired using the Asan Medical Center Coronary Artery Bypass Surgery and Anesthesia Database and the computerized patient record system (Asan Medical Center Information System Electronic Medical Record). This observational study was performed in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
The primary end point was the occurrence of AKI (increase in serum creatinine of ≥0.3 mg/dL or ≥150% from baseline or initiation of renal replacement therapy [RRT]) after CABG. AKI was staged using the AKI Network Classification of changes in serum creatinine concentration within the first 48 hr after operation (13). Data on urine output were not used for diagnosis of AKI due to insufficient recording in all patients and the effects of administered diuretics. RRT was defined as any use of intermittent hemodialysis or continuous venovenous hemodiafiltration. Serum creatinine levels were measured preoperatively, on arrival at the ICU, 6 hr after surgery, and 1 and 2 days after surgery. The concentration that was measured closest to the time of surgery was considered to be the baseline creatinine level. The highest concentration that was measured in the first 48 hr after surgery was used for the primary endpoint evaluation. The preoperative estimated glomerular filtration rate (eGFR) was determined using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (eGFR=141×min (SCr/κ, 1)α×max (SCr/κ, 1)-1.209×0.993age×1.018 [if female]×1.159 [if Black], where SCr is serum creatinine, κ is 0.7 for females and 0.9 for males, α is -0.329 for females and -0.411 for males, min indicates the minimum of SCr/K or 1 and max indicates the maximum of SCr/K or 1) (14). Serum uric acid was measured by an enzymatic method using an automatic biochemistry analyzer (Cobas® 8000 modular analyzer series; Roche Diagnostics GmbH, Vienna, Austria) and the reference range for this uric acid assay at our institution is 3.0-7.0 mg/dL. As previously described (1215), CABG and perioperative management were performed using standard techniques.
Statistical analysis
Continuous variables were reported as mean±standard deviation or median with interquartile range, and categorical variables as numbers and percentages. Univariate comparisons between groups were performed using the chi-square test for categorical variables and Student's t-test or the Mann-Whitney rank-sum test for continuous variables, as appropriate. To test the hypothesis that preoperative uric acid is associated with postoperative AKI, logistic regression analyses were performed. Initially, all preoperative and intraoperative variables in Table 1 were evaluated independently for their possible effect on the occurrence of postoperative AKI. All variables with a P value<0.20 in univariate analysis and some important risk covariates (age, sex, body mass index, diabetes mellitus, hypertension, peripheral vascular disease, preoperative eGFR <60 mL/min/1.73 m2, hematocrit, logistic EuroSCORE, preoperative serum albumin level, use of diuretics, cardiopulmonary bypass time, intraoperative infused crystalloid volume, use of packed red blood cell and platelet concentrate during surgery) were then entered into the multivariate logistic regression model. The final models were determined by backward elimination procedures. The model retention criteria were set at P<0.05. Serum uric acid was analyzed as continuous variable, sex-specific quartiles (i.e., Quartile 1, <4.8 mg/dL for males and <4.2 mg/dL for females; Quartile 2, 4.8-5.5 mg/dL and 4.2-4.9 mg/dL; Quartile 3, 5.6-6.4 mg/dL and 5.0-5.8 mg/dL; Quartile 4, ≥6.5 mg/dL and ≥5.9 mg/dL) and dichotomous variable (i.e., ≥5.6 mg/dL vs. <5.6 mg/dL for males and ≥5.0 mg/dL vs. <5.0 mg/dL for females) based on the distribution of study population.
We conducted further analyses using severe AKI (≥AKI Network stage 2 with RRT) as the outcome and using subgroups of patients. A priori subgroup analysis was performed based on sex, ejection fraction, preoperative eGFR, use of diuretics, and use of cardiopulmonary bypass. For additional analyses, we analyzed uric acid as a continuous variable, and models were constructed as logistic regression identical to the final model above. Adjusted odds ratio (OR) with 95% confidence interval (CI) were calculated to summarize the strength of the association of each variable with postoperative AKI. Model calibration and discrimination ability were evaluated using the Hosmer-Lemeshow goodness-of-fit test and C statistic, respectively.
We evaluated whether the addition of preoperative uric acid improved the predictive ability of our models for AKI in the overall population (model 1), in patients undergoing off-pump CABG (model 2), and in patients undergoing CABG with cardiopulmonary bypass (model 3) by using C statistic, the net reclassification improvement (NRI), and the integrated discrimination improvement (IDI) (1617). CIs for the difference in C statistics between models were calculated by bootstrap resampling. In this study, we used category-free reclassification measure (category-free NRI) due to absence of clinically relevant cut-off values for the risk of AKI after CABG. Reclassification analyses were performed using uric acid as a continuous variable. We also examined the extent of improvement of their predictive value for AKI by adding uric acid in the existing risk model (Northern New England Cardiovascular Disease Study Group [NNECDSG] model) that has been developed to predict AKI after cardiac surgery (18). Risk factors for NNECDSG model included age, sex, diabetes mellitus, white blood cell >12,000, prior CABG, congestive heart failure, peripheral vascular disease, hypertension, and preoperative intraaortic balloon pump.
All reported P values are two-sided, and P values <0.05 were considered statistically significant. SAS® Version 9.1 (SAS Institute Inc., Cary, NC, USA) software was used for all data manipulations and statistical analyses.
RESULTS
Of the 2,308 patients identified, 123 were excluded, including five for not having uric acid and/or creatinine measurements, 87 who underwent preoperative dialysis, 14 who underwent other types of cardiac surgery besides CABG, five with a prior history of organ transplantation or nephrectomy, and 12 who received allopurinol. The remaining 2,185 patients met the study criteria and were analyzed.
The baseline and perioperative characteristics of the study population are shown in Table 1. Mean age was 63.6±9.1 yr and 552 (25.3%) were female. The mean preoperative uric acid concentration was 5.6±1.5 mg/dL (range, 1.0 to 13.8 mg/dL). Of the 2,185 patients, 787 (36.0%) experienced AKI after CABG, including 674 (30.9%) with an AKI Network classification of stage 1, 34 (1.6%) with stage 2, and 79 (3.6%) with stage 3, and 61 patients (2.8%) required RRT. Compared to patients without AKI, patients with AKI were older, had higher logistic EuroSCORE and preoperative creatinine, uric acid and C-reactive protein concentrations, and lower ejection fraction and preoperative hematocrit, total bilirubin and albumin concentrations. Patients with AKI were also more likely to have histories of diabetes mellitus, hypertension, congestive heart failure, cerebrovascular disease, peripheral vascular disease and eGFR <60 mL/min/1.73 m2, and to be receiving angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapy and diuretics. In addition, patients with AKI were more likely to undergo CABG with cardiopulmonary bypass.
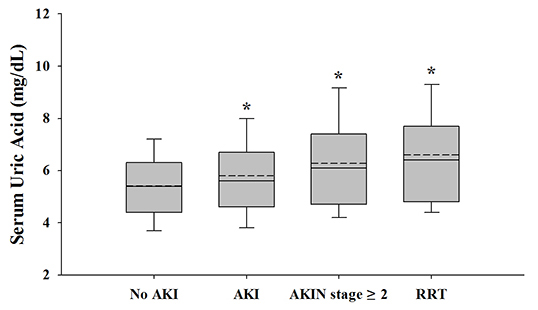
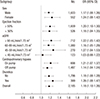
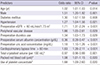
The relationship between postoperative AKI rate and preoperative serum uric acid concentration is shown in Fig. 1. Patients with higher uric acid had a progressively higher incidence of AKI and severe AKI (≥AKI Network stage 2 and RRT). In multivariate analyses, preoperative serum uric acid was a significant predictor of AKI after CABG (OR, 1.18; 95% CI, 1.10-1.26; P<0.001 for continuous variable, OR, 1.53; 95% CI, 1.16-2.01; P=0.003 in quartile 3 and OR, 1.63; 95% CI, 1.24-2.15; P=0.001 in quartile 4 vs. quartile 1, and OR, 1.51; 95% CI, 1.24-1.85; P<0.001 in uric acid ≥5.6 mg/dL for males and ≥5.0 mg/dL for females). Additionally, preoperative serum uric acid was also significantly associated with severe AKI after CABG (OR, 1.19; 95% CI, 1.067-1.35; P=0.003). Other risk factors associated with postoperative AKI were shown in Table 2. As shown in Fig. 2, preoperative uric acid was also significantly related to postoperative AKI in subgroups, except for the subgroup with preoperative eGFR <45 mL/min/1.73 m2.
As listed in Table 3, the addition of preoperative uric acid to the multivariate model (model 1) yielded slightly increases in the significant C statistic for AKI. Moreover, both the category-free NRI (0.216; 95% CI, 0.129-0.302; P<0.001) and the IDI (0.013; 95% CI, 0.008-0.018; P<0.001) were significant for AKI. Adding preoperative uric acid to subgroup and other risk prediction models (model 2, model 3, and NNECDSG model) yielded slightly increased C statistics that were not significant for AKI. However, both the category-free NRI (0.127; 95% CI, 0.022-0.232; P=0.021 in Model 2, 0.306; 95% CI, 0.162-0.450; P<0.001 in Model 3, and 0.177; 95% CI, 0.090-0.264; P<0.001 in NNECDSG model) and the IDI (0.006; 95% CI, 0.002-0.010; P=0.003 in Model 2, 0.014; 95% CI, 0.005-0.024; P<0.001 in Model 3, and 0.013; 95% CI, 0.008-0.017; P<0.001 in NNECDSG model) were significant for AKI in all models.
Of the 2,185 patients, 25 (1.1%) died in-hospital or within 30 days of CABG, with the rate being significantly higher in patients with AKI compared with those without AKI (2.8% vs. 0.2%; P<0.001). The mean durations of stay in the ICU and hospital were 2.7 days and 10.5 days, respectively. Patients with AKI had prolonged extubation time, ICU stay, and hospital stay compared with those without AKI (19.0±33.0 hr vs. 10.1±6.5 hr; P<0.001, 3.6±6.8 days vs. 2.2±1.4 days; P<0.001, and 13.4±21.6 days vs. 8.9±6.4 days; P<0.001, respectively).
DISCUSSION
In this large single-center observational study of 2,185 patients undergoing CABG, preoperatively elevated uric acid concentration was strongly associated with increased risk of postoperative AKI, with the incidence of AKI near linearly increasing with increasing uric acid. Even after adjustment for important preoperative and intraoperative confounders, patients with preoperative elevated serum uric acid were at significantly higher risk of postoperative AKI. Additionally, preoperative uric acid significantly improved risk discrimination and reclassification over the baseline risk models. Furthermore, consistent with previous findings, we also identified that patients with postoperative AKI, despite mild form not requiring RRT in most cases, had a significantly higher mortality rate and poorer outcomes compared with patients without AKI.
Hyperuricemia has been strongly linked to renal disease in various clinical conditions (7), and recent experimental and clinical studies suggest that hyperuricemia may be an independent risk factor for AKI and chronic kidney disease (61920). Despite these strong associations, few studies to date have evaluated the effect of preoperative hyperuricemia on postoperative AKI in patients undergoing cardiac surgery (910). One study, in 58 patients undergoing complicated cardiac surgery, found that preoperative uric acid >6.0 mg/dL was associated with a nearly 4-fold increased risk of AKI and a longer hospital stay than preoperative uric acid ≤6.0 mg/dL (9). Another study, in 190 patients undergoing cardiovascular surgery, found that, after adjustment for confounders by multivariate logistic regression analysis, serum uric acid concentrations ≥7.0 mg/dL were associated with a 35-fold higher risk of AKI, and increased hospital stay and duration of mechanical ventilation support, than serum uric acid concentrations <7.0 mg/dL (10). Our previous study in patients undergoing cardiovascular surgery also found that preoperative hyperuricemia was an independent risk factor of postoperative AKI and was related to poor outcomes (11). Our findings are in agreement with those of the above studies and suggest a similar relationship between preoperative uric acid and postoperative AKI. Our study, however, included a much larger number and more homogeneous population of consecutive patients undergoing CABG, as well as adjusting for a great number of confounders, known as risk factors of AKI in other studies, using a comprehensive and accurate data obtained by data abstractors who were blinded to the objectives of this study. Furthermore, our results were consistent across several subgroups and in the analysis using severe AKI as outcome. These characteristics may enhance the robustness of our results.
Given the growing burden of AKI in patients undergoing CABG, validation of uric acid as a simple and convenient prognostic indicator would be valuable. Most studies assessing renal risk have not included preoperative measure of uric acid. In our study, C statistics increased slightly, albeit significantly, after adding uric acid to the multivariate model in the whole study cohort, whereas the increase did not reach significance in other models. However, C statistic may be relatively an insensitive method to evaluate the impact of adding new predictors to established predictive models (21). In the present study, the improvement in model performance and the added predictive value obtained by adding serum uric acid to the baseline risk models, as gauged by two new metrics (IDI and NRI), which could overcome the limitation of C statistics and quantify risk prediction improvement offered by a new marker, were significant for AKI. Moreover, the additional predictive values of serum uric acid were consistent across existing reference models (NNECDSG models) and models for different subgroup population (CABG with and without cardiopulmonary bypass). These findings indicate that preoperative serum uric acid can improve the predictive ability of established risk prediction models for AKI in patients undergoing CABG.
Serum uric acid is excreted mainly by the kidney, which means that a rise in the serum uric acid level may be inevitable in patients with renal dysfunction. Therefore, whether preoperative elevated uric acid level is simply a marker of preoperative renal dysfunction or whether it is actually responsible for postoperative AKI remains unknown. However, our subgroup analyses showed that, in patients with preoperative normal renal function, preoperative elevated uric acid level was also independently related to the increased risk of postoperative AKI. In addition, several studies suggest that uric acid may itself be a potential contributor to renal injury. Uric acid is reported to impair renal blood flow autoregulation through renal vasoconstriction, which is caused by activation of renin-angiotensin system and inhibition of renal neuronal nitric oxide synthase (7). Uric acid was also shown to induce proinflammatory activities and oxidative stress (72223). Furthermore, our present data show a dose-response relationship between serum uric acid level and the incidence of AKI, which could support the hypothesis of a causal relationship (24). Overall, these observations indicate that hyperuricemia may be causally associated with postoperative AKI rather than just being a simple marker. Thus, preoperative elevated serum uric acid may promote a higher incidence of postprocedural AKI in patients undergoing CABG. Further studies are needed to test this hypothesis.
Our study did not show a J-shaped relationship between serum uric acid and AKI as seen in a previous study (10). This discrepancy may be explained by the difference in baseline characteristics of study populations (ethnicity, cormobidities, or inclusion of off-pump surgery), or differences in perioperative management strategies. In addition, although uric acid has been known to be a major antioxidant and the relative contributions of the individual antioxidants may be different, a decrease in the levels of one antioxidant (i.e., uric acid) could be compensated by other oxidants (25). In other words, a lack of uric acid and its antioxidant capacities, but maintained by other antioxidants, may be associated with lower postoperative AKI in our cohort.
We found that the incidence of post-CABG AKI was higher in patients with serum uric acid ≥5.6 mg/dL for males and ≥5.0 mg/dL for females than <5.6 mg/dL and <5.0 mg/dL, respectively. This cut-off level is well below that usually used to define hyperuricemia. Thus, our results suggest that the association between preoperative hyperuricemia and postoperative AKI is not restricted to the normal range. In other words, elevated preoperative serum uric acid, even when within the normal range, may be associated with a higher risk of postoperative AKI in patients undergoing CABG. These findings are consistent with the results of previous studies, showing that mildly elevated uric acid concentrations within the normal range (≥5.5 mg/dL) have oxidant and inflammatory effects, and were associated with AKI and increased cardiovascular risk (1026). However, the clinical significance of this cut-off value requires validation in larger clinical studies.
Our results may have some important clinical implications. First, measuring preoperative serum uric acid may be of value in identifying patients at high risk for AKI. That is, our findings suggest that patients with preoperatively elevated uric acid could be considered at high risk for AKI. These patients may therefore require intensive monitoring and care during the perioperative period to prevent post-CABG AKI. Second, if the relationship between preoperative hyperuricemia and post-CABG AKI is indeed causal, preoperative hyperuricemia may be a modifiable risk factor. That is, reducing uric acid concentration, especially in patients undergoing elective surgery, may minimize the risk of AKI after CABG. Indeed, several recent small clinical studies showed that uric acid-lowering treatment could slow the progression of renal disease and reduce cardiovascular risk in patients with chronic kidney disease, as well as reducing renal structural injury in patients undergoing cardiovascular surgery (272829). Additional large, prospective, controlled randomized trials may be needed to determine whether hyperuricemia correction prior to CABG improves renal outcome.
The present study has some limitations. First, due to its retrospective, observational design, our findings should be deemed hypothesis-generating, and the causal association between preoperative hyperuricemia and post-CABG AKI not definitively determined. Second, as with any observational study, despite including many variables in our analyses, we could not exclude the effects of other hidden or unknown factors on the observed relationship. Third, although subgroup analyses can provide additional information, issues related to multiple statistical testing, the lack of power, and the occurrence of false positive and/or false negative results may limit these findings. Fourth, despite excluding patients treated with allopurinol, other drug therapy including angiotensin-converting enzyme inhibitor or angiotensin receptor blocker could also affect preoperative serum uric acid levels (30). Thus, we could not exclude the effects of these agents on our results. Additionally, the value of risk models may be dependent on the outcome and the population being examined. The NNECDSG model was originally developed to predict severe renal insufficiency in patients with CABG with a preoperative normal renal function (18). This may explain the lower predictive power compared to C statistic (0.72) shown in original papers. Finally, this was a single-center study performed at a tertiary care academic medical center. Therefore, caution is advised when generalizing these results to centers with different patient profiles.
In conclusion, our current large observational study confirmed that preoperatively elevated serum uric acid was significantly associated with AKI and improved the ability to predict the development of AKI in patients undergoing CABG. Further studies are warranted to evaluate the additional predictive value of serum uric acid in other cohorts and the benefit of preoperatively lowering uric acid levels to reduce postoperative AKI.


 XML Download
XML Download