

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Suicide is one of the significant cause of death in the world (1). An estimated 29.1 persons per 100,000 population die from suicide in South Korea, which is the highest among the Organization for Economic Cooperation and Development (OECD) countries (Korean National Statistical Office, 2012). Many previous studies have investigated for the epidemiological phenomena and the risk factors associated with suicide behavior (234567). Patients who had a previous suicide attempt have a greater possibility to reattempt suicide and also complete suicide (89). That is, the history of attempted suicide is one of the important risk factors for predicting suicide.
In addition, several studies have examined the effect of suicide treatment and suicide prevention programs (10111213). The case management intervention program shed new light on the suicide prevention program for suicide attempters. For example, Szanto, Kalmar (14) examined the effectiveness of general practitioners (GPs)-based depression-management educational program and found that the GP-based program had an effect of decreased suicide rates. In France, 13 emergency departments participated in the study to examine the effects of over one year of contacting patients by telephone (15). They had contacted the patients by telephone at one month or three months after leaving the emergency department (ED) for suicide behavior. Contacting patients by telephone after one month might help reduce the number of suicide reattempts over a year. In Spain, a similar study was also conducted. The study investigated the effectiveness over one year of a telephone management program on patients who attempted suicide (16). The study suggested that a telephone management program would be effective to delay further suicide attempts and reduce the rate of suicide reattempts.
Despite the fact that the suicide prevention case management program is very effective in preventing reattempts, the prevention approaches have shown a major limitation in terms of low participation rates. For example, Vaiva et al.'s (15) study reported a high refusal rate (237/842; 28%), but there were no descriptions about the characteristics of the refusal group. This raised the research necessity to further understand the characteristics of the refusal group. To our understanding, however, no studies have examined characteristics of patients who refused to participate in the case management program after a suicide attempt.
Therefore, the present study compared the characteristics of the refusal group with those of the participation group for the suicide prevention case management program in Korea.
MATERIALS AND METHODS
Study population
A total of 489 suicide attempters who visited Uijeongbu St. Mary's Hospital, the Catholic University of Korea, from December 2009 to December 2013 were included in this study. Patients were eligible if their behavior was confirmed as a suicide attempt by information from the patients themselves, or objective information given by their family, guardians, or rescuers confirmed that the patients had attempted suicide although patients denied a suicide attempt. Patients were excluded if they refused to participate in psychiatric interview, or they could not be interviewed owing to a critical condition caused by their suicide behavior. There was no age limit. All participants consented to interview with a psychiatric resident in the emergency ward. After diagnostic interview by psychiatry residents, patients were introduced to the case management program for suicide attempters. The case management program included information, education, and practical advice through brief interventions with the maintenance of long-term follow-up telephone contact on a regular basis.
Among them, 262 patients agreed to participate in the case management program (participation group) and 227 patients refused to participate (refusal group).
Procedures and assessment instruments
All patients were assessed in the emergency room using the Brief Emergency Room Suicide Risk Assessment (BESRA) (567). It contains patient's demographic variables (age, sex, marriage, religion, psychiatric family history), clinical characteristics (agitation, medical illness, severity depression, nature of suicide ideation), and factors related to the presenting suicide behavior (number of suicide attempts, planning, precipitating events, insight of suicide attempt, hopelessness/helplessness, intention, regret, interpersonal relationship, and social integrity). Medical severity was assessed by a clinician using the 'method and lethality of method' item of Suicide Attempt Self-Injury Interview (SASII) developed by Linehan (17). The score of items measuring medical severity ranged from level 1 to 6 (1=very low, 2=low, 3=moderate, 4=high, 5=very high, and 6=severe). The clinician also assessed lethality by measuring risk-rescue rating developed by Weisman and Worden (18). Psychiatric residents in the emergency ward conducted the psychiatric interview using DSM-IV-TR and BESRA. To ensure that all the psychiatry residents were well informed of the BESRA and performed aptly, two psychiatry specialists (a professor and a clinical instructor of psychiatry) instructed them. Furthermore, consensus meetings were held biweekly under the supervision of the same two psychiatry specialists.
Statistical analysis
Demographic and clinical characteristics of each group were summarized and are presented as mean±standard deviation, frequency or percentage depending on the variable types. Patients were divided into two groups (participation vs. refusal group) based on the patients' agreement on the case management program. T-tests and chi-square analyses were conducted on all variables comparing two groups. All statistical analyses were performed by SAS/PC version 9.2 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Demographic characteristics
All data of the 489 patients were analyzed. Table 1 shows the overall characteristics of the data. The mean age between the two groups was not different (45.5±17.6 vs. 44±17.5 yr, the participation vs. the refusal group, respectively). A total of 262 (53.6%) patients were included in the participation group and 227 (46.4%) patients were in the refusal group. In the participation group, 92 patients (35.1%) were male, and 170 patients (64.9%) were female. Ninety-four males (41.4%) and 133 females (58.6%) were in the refusal group. The refusal group had more patients who did not have religion (88.5% vs. 82.1%, the participation group vs. the refusal group, respectively, P=0.045). Sex, marriage, employment and socioeconomic status had no significant differences between the two groups.
Clinical characteristics
In total, the most common psychiatric diagnosis was major depressive disorder (n=259, 45.9%) followed by depressive disorder (n=115, 20.4%), adjustment disorder (n=91, 16.1%), alcohol-related disorder (n=38, 6.7%), bipolar depression (n=20, 3.5%), schizophrenia and other psychotic disorder (n=18, 3.1%) and others including anxiety disorder, impulse control disorders, somatoform disorders, sleep disorders, eating disorders, and childhood psychiatric disorders. There were no significant differences on the psychiatric diagnoses between the two groups. However, the refusal group tended to include less percentage of patients with major depressive disorder 111 (41.9%) vs. 148 (49.5%), the refusal vs. participation group (P=0.07).
The refusal group had significantly less co-morbid medical illnesses compared to the participation group (21.7% vs. 37.4%, the refusal vs. participation group, respectively, P<0.001). Regarding the severity of depression, more patients with mild depression were included in the refusal group than the participation group (13.2% vs. 6.5%, the refusal vs. participation group, respectively, P=0.031). 'Rare/mild/transient' nature of suicide ideation was more common in the refusal group than the participation group (56.8% vs. 46.6%, the refusal vs. participation group, respectively, P=0.024), while 'repetitive/intense/continuous' nature of suicide ideation was more common in the participation group than the refusal group (53.4% vs. 43.2%, the participation vs. refusal group, respectively, P=0.024).
Factors related with the presenting suicide behaviors
The most common method of suicide attempt was overdose (n=385, 80.4%) followed by cut (n=57, 11.9%), hanging (n=16, 3.3%), CO poisoning (n=14, 2.9%), jumping (n=6, 1.3%), and traffic accident (n=1, 0.2%). Although there were no significant differences on the suicide methods between the two groups, CO intoxication tended to be a less frequent method of suicide for the refusal group than the participation group 3 (1.3%) vs. 11 (4.2%), for the refusal vs. participation group, (P=0.063). The mean of the total rescue scores for the refusal group was significantly higher than that of the participation group (12.8±1.9 vs. 12.4±1.9, the refusal vs. participation group, respectively, P=0.024), whereas the mean of the total risk scores was not different between the two groups. Medical severity of the refusal group was significantly lower than that of the participation group (3.0±1.1 vs. 3.2±1.1, the refusal vs. participation group, respectively, P=0.024).
More patients in the refusal group than the participation group had impulsive suicide attempts (93% vs. 85.5%, the refusal vs. participation group, respectively, P=0.009) and impaired insight about their suicide behavior (87.7% vs. 80.2%, the refusal vs. participation group, respectively, P=0.025). The refusal group was less likely than the participation group to have hopelessness/helplessness (61.2% vs. 71%, the refusal vs. participation group, respectively, P=0.019).
In addition, the refusal group had more common conflictual interpersonal relationships (76.7% vs. 63.7%, the refusal vs. participation group, respectively, P=0.002) and social isolation (74.4% vs. 61.8%, the refusal vs. participation group, respectively, P=0.003).
Reasons for the refusal
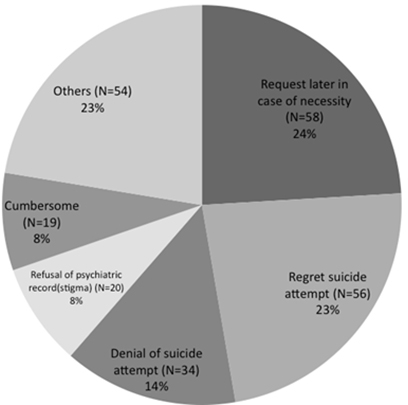
Analysis of reasons for the refusal of participation in the case management program was conducted only for the refusal group. Fig. 1 shows the reasons for the refusal of participation. "Request later in case of necessity" (24%) was the most common reasons for the refusal to participate in the case management program. "Regret suicide attempt" (23%) was the second reason for the refusal, followed by "denial of suicide attempt" (14%), "refusal of psychiatric record due to stigma" (8%) and "cumbersome" (8%). Other reasons (23%) were "want to visit clinic near home", "want to visit clinic where patients already followed up" and "no reason."
DISCUSSION
The present study revealed characteristic features of patients who refused to participate in the suicide prevention case management program after attempting suicide in Korea. The present study showed a high rate (46.4%) of nonparticipation in the case management program. Given that previous studies have demonstrated the effectiveness of case management programs (141516), the high rate of nonparticipation in the case management program is disappointing. The nonparticipation rate of the present study was higher compared to 28% of Vaiva et al.'s study (15). It is difficult to compare reasons for this discrepancy because no information is available from Vaiva et al.'s study (15). However, this might be explained by multiple compliance factors such as patient-centered factors, therapy-related factors, social and economic factors, healthcare system, and disease factors (19).
Interestingly, the present study revealed low risks for suicide in the refusal group in terms of risk factors related with psychopathologies and presenting suicide behavior. That is, the refusal group had less co-morbid medical illnesses and more patients with mild severity of depression compared to the participation group. In addition, they had less serious suicide ideation that was rare, mild and transient. The refusal group attempted suicide in a more rescuable way and less severe way in medical severity.
Given that serious psychopathologies and medical illnesses increased the risk of suicide (5), the findings of the present study may suggest more favorable outcomes of the refusal group in terms of the current suicide attempt and future suicide reattempts. However, the risk for suicide reattempt may not be less in the refusal group, since previous history of suicide attempt increases the risk for suicide reattempt (89) and only less than half of the refusal group regretted their suicide attempt and wanted follow-up at their previous clinic (Fig. 1). Over half of the patients in the refusal group had reasons for nonparticipation the suicide prevention case management program related to poor insight. Such reasons for nonparticipation were 'request later in case of necessity', 'denial of suicide attempt', 'refusal of psychiatric medical record due to stigma', and 'cumbersome'. This finding explains why more patients in the refusal group showed poor insight about their suicide attempt (Table 1). The lack of insight about the suicide attempt may lead to the refusal of participation in the suicide prevention case management program. Insight has an important role in psychological treatment in various mental disorders (202122). Patients having insight are more likely to accept treatment than those without insight. Treatment compliance has been considered in most studies to be strongly correlated to insight. In other words, poor insight leads to poor compliance and further influences poor therapeutic outcomes as well (23). Therefore, emergency suicide interviews focused on improving insight of the patients may facilitate patients' participation in the case management program and thus improve the outcome.
The current finding that more patients in the refusal group had conflictual interpersonal relationships may also suggest poor outcomes of this group. More patients in the refusal group had not only conflictual interpersonal relationships but also isolation in social integrity. These difficulties imply the lack of social support for the refusal group. Social support plays a key role as the protective factor to improve resilience in the context of daily stress (24). In this respect, the refusal group with lack of social support may have higher possibility to reattempt suicide. Previous studies have also suggested that interpersonal relationship problems may significantly increase the risk for suicide reattempt (25). Thus, furthermore, suicide prevention case management programs that provide social support may contribute to reduce suicide reattempts (26).
The present study has some limitations. The population of the present study is limited to one university hospital in a specific area in Korea, which may limit generalization of the findings of the current study. In addition, caution should be made when interpreting the findings of the current study, since there was selection bias due to patients who refused to consent to psychiatric interviews. The authors focused on the demographic, clinical characteristics that might impact nonparticipation in the case management program. Thus, investigating other factors that might influence compliance may further expand our understanding of the refusal group for the suicide prevention program. Given the above limitations of the current study, we believe the findings of the current study may shed more light on the understanding of the suicide behavior and provide more insights on planning suicide prevention programs.
In conclusion, patients with a suicide attempt who refused to participate in the suicide prevention case management program showed less serious suicide attempts and medical and psychiatric problems. However, impaired insight of the suicide attempt and lack of social support may suggest poor outcomes of the refusal group.


 XML Download
XML Download