

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Histologic chorioamnionitis (HC) is characterized by a maternal inflammatory response that involves neutrophil infiltration in the fetal membranes and/or placenta with or without a fetal inflammatory response (FIR), which is indicated by funisitis (1). HC is a reliable marker for ascending genital tract infection and is a major risk factor for preterm birth and prematurity-associated morbidities (2345678). There have been not a few studies supporting the adverse effects of HC on neonatal outcomes, but controversies continue on this issue.
A recent systematic review of 59 studies reported that the definition of chorioamnionitis varied across the studies (9). Different studies used different definitions; therefore, the true effects of HC have been confounded by the absence of a uniform definition and standardized histologic diagnostic criteria. The current definition of HC encompasses amnionitis, choriodeciduitis, funisitis, and placental inflammation (10). The fetal and neonatal impact of HC may be different by the site of inflammation within the uterus. The FIR associated with HC has been known to contribute to adverse neonatal outcomes (11). Yoon et al. (1) reported that funisitis is associated with amniotic fluid infections, neonatal sepsis, and FIR syndrome. Amnionitis is the final stage of extra-placental chorioamniotic inflammation. Park et al. (12) demonstrated that the involvement of amnion in the inflammatory process is associated with a more intense fetal and intra-amniotic inflammatory responses compared with chorionitis alone. In this regard, we focused on funisitis and amnionitis in defining HC. Moreover, not only the site of inflammation but also the extent of inflammation at each site maybe related with fetal and neonatal consequences of HC. Therefore we sub-defined high grade inflammation in each site of HC. The aim of this study was to determine the relationship between HC and neonatal morbidities in very low birth weight (VLBW) infants using the definition of HC that reflects both the site and extent of inflammation.
MATERIALS AND METHODS
Subjects
This study included all VLBW infants with a birth weight of <1,500 g who were born and admitted at the neonatal intensive care unit at Seoul National University Bundang Hospital between January 2008 and December 2012. We excluded infants with major congenital anomalies and infants whose placentas were not available for pathologic assessment.
Definitions of histologic chorioamnionitis
Placentas are routinely sent for histologic examination immediately after preterm delivery at our center. HC was diagnosed by the presence of acute inflammation and infiltration of polymorphonuclear leukocytes (PMN) in the amnion, chorionic decidua, umbilical cord, or the chorionic plate; and was divided into four grades depending on the extent of PMN infiltration using the grading system devised by Salafia et al. (13) by a single pathologist (Table 1). Based on the histological findings described according to this grading system, we defined HC into four categories based on the site and extent of PMN infiltration: PMN infiltration of any grade in any part of the amnion, chorionic decidua, umbilical cord, and chorionic plate was defined as any HC; PMN infiltration of any grade in the amnion as amnionitis; PMN infiltration of any grade in the umbilical cord as funisitis; and PMN infiltration of any grade in both the amnion and umbilical cord as amnionitis plus funisitis. Furthermore, the extent of PMN infiltration of grade 3 or higher at each site of inflammation was sub-defined as high grade (HG) (Table 1). We compared the incidences of neonatal morbidities between the VLBW infants with or without HC using the above definitions of HC.
Definitions of clinical terms
Antenatal, perinatal, and neonatal data were retrospectively collected from the original medical records of the infants included in this study. The retrieved data included maternal age, type of delivery, antenatal steroid use, premature rupture of membranes (PROM) >18 hr, antenatal antibiotic use, the clinical and histologic diagnosis of chorioamnionitis, maternal preeclampsia, gestational age (GA), birth weight, gender, multiple births, small for gestational age (SGA), and Apgar scores at 1 and 5 min. Clinical chorioamnionitis was diagnosed by the presence of a fever of 38.3℃ or higher, and the presence of at least two of the following: leukocytosis (>18,000/µL), vaginal discharge with foul odor, uterine sensitivity, and tachycardia (maternal >100/min, fetal >180/min). SGA was defined as a birth weight below the 10th percentile for GA. Neonatal morbidities included respiratory distress syndrome (RDS), defined by the presence of respiratory distress, as indicated by an increased oxygen requirement (FiO2≥0.4) and compatible chest radiographic findings without any evidence of another cause of respiratory distress; bronchopulmonary dysplasia (BPD), defined as supplemental oxygen dependency at 36th week postmenstrual age; early-onset sepsis (EOS) and late-onset sepsis (LOS), defined as a systemic bacterial infection documented by a positive blood culture within the first 72 hr of life or after the first 72 hr of life, respectively, with a clinical presentation consistent with sepsis; intraventricular hemorrhage (IVH) and periventricular leukomalacia (PVL), diagnosed via cranial ultrasonography; necrotizing enterocolitis (NEC), defined according to Bell's criteria (14); and retinopathy of prematurity (ROP), defined based on the International Classification of ROP.
Statistical analysis
Statistical analyses were performed using the SPSS software, Version 21.0 (SPSS, Inc., Chicago, IL, USA). Continuous variables were expressed as means and standard deviations or as medians and interquartile ranges, and were analyzed using either Student's t-test or the Mann-Whitney U-test. Categorical variables were expressed as proportions (%), and chi-square or Fisher's exact tests (two-sided) were used for comparisons. Logistic regression analysis was performed to adjust for both GA and birth weight. Adjusted odds ratios (aOR) and 95% confidence intervals (CI) were reported, and a P value <0.05 was considered statistically significant.
RESULTS
Subjects enrolled
During the study period, 261 VLBW infants were born and admitted at our neonatal intensive care unit, and their eligibility to participate in the study was assessed. Among them, two infants with insufficient placental histologic data and one infant with congenital anomaly were excluded.
Histologic chorioamnionitis based on the site of inflammation
Of the remaining 258 infants, 99 (38.4%) infants were exposed to any HC. The demographic and perinatal characteristics of the VLBW infants who were exposed and not exposed to HC based on the site of inflammation are shown in Table 2. Mothers with HC were more likely to have PROM and clinical chorioamnionitis, receive antibiotics, and deliver vaginally. Mothers without HC were more likely to have preeclampsia. The mean GA was significantly lower in the HC-exposed infants in all sites of inflammation. The HC-exposed infants were more likely to be of singleton and less likely to be SGA. There were no significant differences in the maternal age, antenatal steroid exposure rate, birth weight, sex, and Apgar scores at 1 and 5 min between the HC-exposed and unexposed infants in all sites of inflammation. The mortality and neonatal morbidities between the HC-exposed and unexposed VLBW infants were shown in Table 3. Twenty five (9.7%) infants out of a total of 258 died within 28 days of birth, and there were no differences in the mortality rates between the HC-exposed and unexposed infants in all sites of inflammation. The incidences of RDS, NEC, IVH of ≥grade 3, PVL, EOS and LOS were not different between HC-exposed and unexposed infants in all sites of inflammation either. However, the incidence of BPD was higher in amnionitis-exposed infants (50% vs. 23.6%, P=0.02). Severe ROP (≥stage 3) and the need for laser surgery were significantly associated with any HC and funisitis (Table 3).
Histologic chorioamnionitis based on the extent of inflammation
Although further analysis on the sub-definitions of HG HC was carried out to observe whether the extent of inflammation in each site further affects the morbidity and mortality of the VLBW infants, there was no significant finding except that BPD occurred more often in infants who were exposed to HG amnionitis than who were not (66.7% vs. 24.0%, P=0.01) (Table 4).
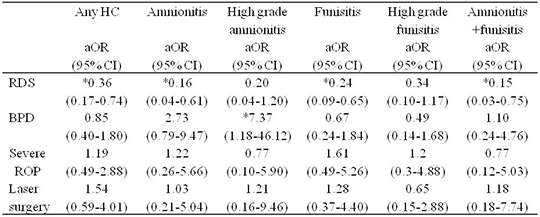
Independent association with neonatal morbidities
We performed further analysis to adjust for both GA and birth weight using logistic regression model (Table 5). After adjustment, the RDS was significantly fewer in HC-exposed infants than in HC-unexposed infants except for the infants who were exposed to HG amnionitis and HG funisitis. Although analysis included HG amnionitis plus funisitis, there was only one case of HG amnionitis plus funisitis, therefore statistical analysis was irrelevant. The incidence of BPD was higher only in infants who were exposed to HG amnionitis than who were not (aOR, 7.37; 95% CI, 1.18-46.12). The relationship of HC with severe ROP and the need for laser surgery disappeared after adjustment for GA and birth weight (Table 5).
DISCUSSION
The primary findings in the present study include a significant association of HC with a reduced incidence of RDS and HG amnionitis with an increased incidence of BPD. Other neonatal morbidities were not associated with HC following adjustment for GA and birth weight. Because the GA was significantly lower in the VLBW infants exposed to HC, adjustment for GA as well as birth weight was needed.
Many studies have supported the idea that HC protects against RDS. Watterberg et al. (15) observed that the increased production of inflammatory cytokines and cortisol accelerate lung maturation and that this process decreases the incidence of RDS. Since the beginning of the era of antenatal steroid treatment, several studies have reexamined the effects of HC. Lahra et al. (16) demonstrated that HC was associated with a significant reduction of RDS; chorioamnionitis with umbilical vasculitis is particularly associated with a markedly reduced incidence of RDS compared with chorioamnionitis alone. Other studies have also described a reduction of RDS among the HC-exposed preterm infants (34). In those studies, the antenatal steroid exposure rate was not different between the HC-exposed and unexposed infants. In the present study, antenatal steroid exposure rate was not different between the HC-exposed and unexposed infants in all site of inflammation either. When adjusted for GA and birth weight, any HC, amnionitis, funisitis, and amnionitis plus funisitis were all significantly associated with a decreased incidence of RDS. These findings support the idea that HC still has a beneficial effect that protects RDS in the era of antenatal steroid treatment. It deserves special mention that HG amnionitis and HG funisitis were not associated with a reduced incidence of RDS. In our previous retrospective cohort study, more severe HC led to RDS and alter the response to surfactant (17). High grade chorioamnionitis may cause a pneumonia in the fetus and newborn preterm infants which is not distinguished clinically from RDS (18). The absence of significant association of HG amnionitis and HG funisitis with the reduced incidence of RDS supports the idea that more severe chorioamnionitis may offset the beneficial effect of HC.
The relationship between chorioamnionitis and BPD is still controversial. The most recent evidence suggests that a maturational effect exerted by HC appears to decrease the incidence of RDS in preterm infants but also contribute to the increased susceptibility to postnatal lung injury (5151920). One study demonstrated that exposure to both HC with/without funisitis and prolonged mechanical ventilation increased the risk of BPD (21) while another study suggested funisitis is protective for BPD (22). A recent systematic review by Hartling et al. (9) showed that HC is significantly associated with the increased incidence of BPD. However, the definition of HC was not consistent across all studies and the authors found a strong evidence of publication bias, which makes the association of HC with BPD inauthentic. In the present study, BPD was not associated with HC of any sites except for HG amnionitis. High grade amnionitis was significantly associated with BPD even after adjustment for GA and birth weight while HG funisitis was not. The reason for this result is unclear but may be related to the observation that severe amnionitis is strongly associated with an intense intra-amniotic inflammatory process (12). Considering the location of the amnion that lines the amniotic cavity, HG amnionitis may portray the presence of a strong chemotactic stimuli present within the amniotic cavity. Several studies unveiled an association between elevated concentrations of pro-inflammatory cytokines in the amniotic fluid and the development of BPD (23242526). Although the underlying inflammatory mechanisms of HC are not fully understood, pro-inflammatory cytokines aspirated by the fetus can directly contact with respiratory epithelium and induce pulmonary inflammation. Fetal pulmonary inflammation can inactivate surfactant and make the lung more susceptible for further injury from oxygen toxicity or mechanical ventilation eventually leading to BPD. The finding that HG amnionitis but not HG funisitis was associated with BPD suggests that fetal pulmonary inflammation via direct contact with the airway epithelium might be more responsible for the development of BPD than fetal systemic inflammation via umbilical cord.
A number of studies have attempted to evaluate the relationship between HC and ROP. Dammann et al. (27) found evidence supporting the idea that extreme prematurity and multiple hits of perinatal inflammation may contribute to an increased risk of ROP. In contrast, Woo et al. (28) reported that neither HC nor funisitis were associated with ROP. A recent systematic review reported that chorioamnionitis was significantly associated with severe ROP. However, the relationship disappeared after adjustment for GA; the authors concluded that chorioamnionitis cannot be considered a definitive risk factor for ROP (29). Our study also found that the relationship of HC with severe ROP and an increased incidence of laser surgery disappeared following adjustment for GA and birth weight.
The limitations of this study include that this is a single center study and is of retrospective nature. The strengths of this study include: the histological diagnosis of chorioamnionitis was made via a consistent standardized placental assessment by a single pathologist; the definition of HC reflected both the site and extent of inflammation; the study was performed in the era of prenatal steroid treatment.
In conclusion, the results of the present study show that HC significantly decreased the incidence of RDS and HG amnionitis increased the incidence of BPD in VLBW infants while lacking association with other neonatal morbidities. These results suggest that the association with HC and neonatal morbidities may differ by the site and extent of chorioamnionitis. We suggest that it is not simply the presence or absence of HC but both the location and severity of HC that correlates with adverse neonatal outcomes. Further studies designed to evaluate the interactions of HC with various postnatal factors are necessary.



 XML Download
XML Download