

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rotavirus (RV) is one of the most important viral agents causing acute gastroenteritis (AGE) in children, although the importance of norovirus (NV) as a causative agent for AGE is increasing (12). Recently, two RV vaccines (RVVs), Rotarix® (GlaxoSmithKlein Co., Middlesex, UK) and RotaTeq® (Merck Sharp & Dohme Co., NJ, USA) were developed. Based on the results of several clinical efficacy studies, these vaccines have been used in young infants to prevent RV infection (345). Postmarketing surveillance studies revealed that the introduction of RVVs has resulted in a significant decrease in AGE due to RV infection in children (6789). In Korea, the RVV is optional and not covered by health insurance. G1, G9, and G3 genotypes have been shown to be predominant in previous Korea studies, with variations observed according to region and study period (101112). In Brazil, the possibility of immune selection due to mass vaccination has been suggested (13), although there are still ongoing debates concerning possible genotypic differences after introduction of RVVs (141516171819). However, the emergence of novel genotypes and outbreaks of rare combinations of genotypes have been observed in recent years (13202122), suggesting the necessity for continued monitoring of RV strains to ensure vaccine efficacy.
The purpose of this study was to investigate RV genotypes five years after introduction of RVVs and to determine the differences in genotype distributions according to vaccination status and vaccine type.
MATERIALS AND METHODS
Study population
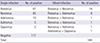
A total of 448 children hospitalized with AGE between October 2012 and September 2013 at 9 medical institutions from 8 provinces: Sanggyepaik Hospital (117 cases in North Seoul, Inje University College of Medicine); Seoul St. Mary's Hospital in South Seoul, 27; Incheon St. Mary's Hospital in Incheon, 18; St. Vincent's Hospital in Suwon, 38; Daejeon St. Mary's Hospital, Catholic University of Korea in Daejeon, 71; Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine in Wonju, 55; Pusan National University Yangsan Hospital, Yangsan, 53; Chonbuk National University Hospital in Jeonju, 33; Changwon Fatima Hospital in Changwon, 42.
The definition of AGE was as follows: 1) loose or watery stool three or more times within 24 hr; 2) abnormal stool associated with fever, severe abdominal pain, or vomiting; and 3) onset of symptoms within 7 days, with the above symptoms being absent 2 weeks before admission. The exclusion criteria for AGE symptoms were as follows: abnormal stool associated with 1) previously diagnosed diseases such as pneumonia or acute otitis media, 2) underlying chronic gastrointestinal diseases, and 3) nosocomial infections (with acute vomiting or diarrhea beginning 48 h after admission). At admission, information for RV immunization status and RVV type were collected from the patient's parents and verified by vaccination cards.
Sample collection and preparation
Stool samples were collected from 417 of 448 hospitalized children with AGE with informed and written consent from the patient's parents. Of 417 stool samples, 346 samples (83.0%) were included in this study, and 71 samples were excluded for the following reasons: other diagnosis (2 cases), age over 5 yr (12 cases), and incomplete case report form (57 cases). Stool samples were stored at -70℃. For experimental use, 1 g of stool was thawed, diluted 1:10 in phosphate-buffered saline (9 mL), vortexed, and centrifuged at 3,200 rpm for 20 min at 4℃. Supernatants were collected for subsequent experiments.
Enzyme-linked immunosorbent assay (ELISA) for identification of RV
RV was initially identified using a BioTracer Rotavirus ELISA kit (Bio Focus Co., Uiwang, Korea) according to the manufacturer's instructions. Stool supernatants (100 µL) and enzyme-conjugated antibodies (100 µL) were added to the plate and incubated for 60 min at 37℃. The positive control was 100 µL of the prepared sample in the ELISA kit, and the negative control was 100 µL PBS. After washing the plate five times with 200 µL PBS using an ELISA washing machine, 100 µL of reagent was added in a dark room for 15 min at room temperature, and 50 µL of stop solution was then added. Sample optical density was measured with an ELISA plate reader at a wavelength of 450 nm and analyzed according to the manufacturer's instructions.
Reverse transcription polymerase chain reaction (RT-PCR) for identification of RV
Total RNA was extracted from stool samples with the QIAamp viral RNA kit (Qiagen GmbH, Hilden, Germany). Multiplex RT-PCR was performed for RV-positive stool samples screened by ELISA, with primers for G-type (G1-G4, G8, and G9) and P-type (P1A[8], P1B[4], P2[6], P3[9], P4[10]), as described previously (23)].
Detection of other enteric viral agents
NV was identified by real-time RT-PCR and conventional nested RT-PCR, as described previously (24). Enteric adenovirus (AdV) was detected with the BioTracer Adenovirus ELISA kit (Bio Focus Co.) according to the manufacturer's instructions. The supernatant conjugate (100 µL) was mixed in each microwell plate and reacted for 1 hr at 37℃. One hundred microliters of test sample from the kit was used as a positive control, and PBS was used as a negative control. The microwell was washed five times with 200 µL PBS. After adding 100 µL of substrate to each microwell and incubating at 20-30℃ for 15 min, 50 µL of stop solution was added to each microwell. Absorbance was read with an ELISA reader at 450 nm.
Astrovirus (AsV) and sapovirus (SV) were detected with the AccuPower Astro-Sapovirus Real Time RT-PCR Kit (BIONEER, Daejeon, Korea). Twenty microliters of RNA sample was added to a PCR tube and centrifuged. Reactions were carried out with an initial reverse transcription step at 48℃ for 40 min, followed by 45 cycles of amplification (30 sec at 94℃, 30 sec at 58℃, and 60 sec at 72℃), and a final extension of 7 min at 72℃. PCR products were run on a 1% agarose gels, stained with ethidium bromide, and visualized under ultraviolet light.
RESULTS
RV detection
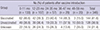
The age distribution of the 346 children in this study was as follows: under 2 months of age in 6.9% (24 cases), 2-5 months of age in 8.1% (28), 6-23 months of age in 53.5% (185), and 24-59 months of age in 30.6% (106). The sex ratio was 1.23 (male to female), 191 males and 155 females. Of 346 stool samples, enteric viral agents were detected in 66.2% (229 cases). RV was detected in 87 cases (38.0%), NV was detected in 95 (41.5%), enteric AdV was detected in 10 (4.4%), AsV was detected in five (2.2%), SV was detected in two (0.9%), and mixed infection was detected in 30 (13.1%; Table 1).
Among the 114 children identified as RV positive by ELISA, single infection of RV occurred in 87 cases (76.3%) while mixed infection with other viruses occurred in 27 (23.7%). The average age of RV-infected patients with AGE was 19.8±13.6 months (median, 16 months). When comparing the ratio of RV-infected patients with AGE to all patients with AGE, there was no statistically significant difference between age groups: 20.3% (27/133) in patients ages 0-11 months, 34.6% (37/107) in patients ages 12-23 months, 29.8% (17/57) in patients ages 24-35 months, 31.0% (9/29) in patients ages 36-47 months, and 25% (5/20) in patients ages 48-59 months. During the study period, RV detection peaked in March and April, but rapidly decreased in May. Mixed infections were frequently observed in October and December.
Vaccination history
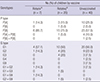
Out of 346 children, vaccination history was available in only 272; vaccinated 144 (52.9%), unvaccinated 128 (47.1%). In the 144 vaccinated children, Rotarix was used for 55 (38.2%), RotaTeq in 73 (50.7%), and an unknown type of RVV in 16 (11.1%). The vaccination rate with RVVs according to age was as follows: 0-11 months, 55.9% (62/111); 12-23 months, 51.9% (42/81); 24-35 months, 54.8% (23/42); 36-47 months, 56.0% (14/25); and 48-59 months, 23.1% (3/13), as shown in Table 2. RV was detected in 27.8% (40/144) of children in the vaccinated group and 39.8% of (51/128) of children in the unvaccinated group (P=0.035).
Genotyping of RV
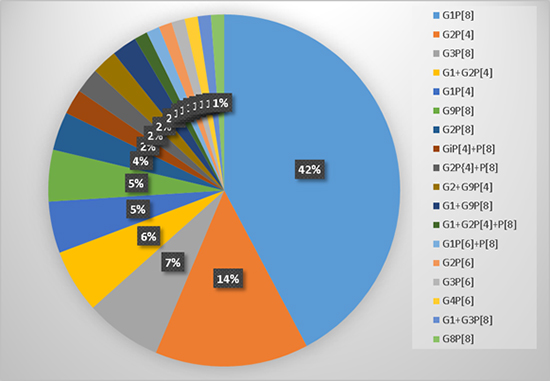
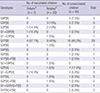
Eighty-six of 114 RV-positive stool samples were successfully genotyped. The most common combinations of genotypes were G1P[8] (36 cases, 41.9%), G2P[4] (12, 14.0%), and G3P[8] (6, 7.0%). Vaccination histories of RVV were available in only 67 of 86 RV genotyped children (Rotarix in seven cases, RotaTeq in 20, and unvaccinated in 40). In 67 RV-genotyped children with known vaccination history, the most common genotypes were G1P[8] (34 cases, 43.3%), G2P[4] (8, 11.9%), G3P[8] (6, 8.9%), and G9P[8] (4, 5.9%). In both vaccinated and unvaccinated children, the most predominant G and P genotypes were G1 and P[8], respectively (Table 3). The most common combination of G/P genotypes was G1P[8]: 57.1% in Rotarix-vaccinated children, 45% in RotaTeq-vaccinated children, and 40% in unvaccinated children (Table 4). In children under 2 months of age which was RV (16.6%, 4/24 cases), the detected genotype was as follows: G1P[8] in 2 cases, G1P[6]P[8] in 1, and G3P[8] in 1.
DISCUSSION
In this study, 32.9% (114/346) of the study population was RV positive. This result was similar to that (29.3%) of a recent Korean study (11). The detection rate of RV in vaccinated group children was significantly lower than that in unvaccinated children, which was consistent with the results of previous studies showing the effects of vaccination on prevention of severe RV-dependent AGE (78925). In Korea, RotaTeq was introduced in June 2007, while Rotarix was introduced in March 2008. After the introduction of these vaccines in Korea, the vaccination rate was reported to be about 30% in 2009, reaching 50.2% [Rotarix-34.1%, RotaTeq-26.1%] in 2012 (2627). Among patients in this study, the RV vaccination rate was 52.9% (144/272), a notable increase in the vaccination rate compared to that in previous studies (2627). It is unclear whether the RV vaccination rate in Korea has actually increased or whether the observed increase in this study may reflect population differences, specifically in residents in major cities, between this study and a report of the vaccination rate in 2012 (27). The most commonly detected RV genotypes in humans are G1-G4, G9, and P[8], and rare combinations of G/P genotypes (G2P[6], G8P[14], and G9P[10]) are frequently observed in undeveloped countries (2829), suggesting that prevalent genotypes vary depending on the year, region, and country of origin. Emergence of the previously rare G9P[4] genotype was reported in Latin America in 2009-2010, suggesting genetic re-assortment (1322), but further epidemiological studies are required to confirm this finding. The predominance of G2P[4] after the introduction of Rotarix was regarded initially as a possible case of the immune escape phenomenon, although this is still debatable (1415171819). In this study, G1P[8] (41.9%) and G2P[4] (14.0%) were the predominant strains among the 86 genotyped RV strains. These data suggested that the prevalent genotypes of RV have not changed after introduction of vaccines in Korea. Furthermore, the G9P[4] genotype was not observed, although some unusual genotype combinations, including P[6] with G2, G3, or G9, were detected. In this study, mixed infections were found (10%) in unvaccinated group. This finding might be a cause of strain diversity of circulating RV, which was suggested in a recent study in India (3031). The limitations of this study include the small size of the study population, the unknown genotypes of excluded cases, and the method of genotyping (multiplex RT-PCR not including G10 and G12).
In conclusion, the RV infection season was delayed by approximately 2-4 months after the introduction of RVVs. The distribution of RV genotypes between vaccinated and unvaccinated groups, however, was not different. These results suggest that RV vaccination may not have driven the emergence of variant RV genotypes by substitution due to immune pressure in Korea during 2012-2013; however, the limitation of this study, including the small sample size and the restricted time-frame, should be considered when analyzing these results.
 XML Download
XML Download