

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pulmonary hyperinflation occurs due to the decreased elasticity of the lung parenchyma, increased airway resistance, and air trapping, as chronic obstructive pulmonary disease (COPD) progresses (12). Many trials have shown that pulmonary hyperinflation significantly impairs breathing and reducing pulmonary hyperinflation has beneficial effects in COPD, as shown by the recent papers that significant improvements in pulmonary function, exercise capacity, and quality of life result from lung volume reduction surgery (345678).
Recent reports also suggested that symptoms and exercise capacity in COPD correlate better with variables related to pulmonary hyperinflation than with forced expiratory volume in 1 second (FEV1), because pulmonary hyperinflation can increase the work of breathing and cause diaphragm dysfunction (2910).
Dynamic hyperinflation has been considered a major contributor to reduced quality of life and poor exercise capacity in COPD (21011). However, static hyperinflation, as expressed by the inspiratory capacity (IC)/total lung capacity (TLC) ratio, is reported to be an independent predictor of mortality in COPD (3). Some papers suggested that residual volume (RV)/TLC is a risk factor for mortality (67). Furthermore, the lung volumes representing resting pulmonary hyperinflation can be easily measured, in contrast to difficult measurement of dynamic hyperinflation. Thus, variables of static hyperinflation are thought to be significant clinical markers of COPD prognosis. However, the prognostic role of RV/TLC representing resting pulmonary hyperinflation was not well explored so far. Therefore, this study was performed to identify the variables that associate with RV/TLC severity and to examine the role of RV/TLC as a COPD prognostic factor.
MATERIALS AND METHODS
Study design
Patients
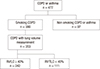
This study involved the Korean Obstructive Lung Disease (KOLD) cohort, which consists of 477 patients with COPD or asthma enrolled from pulmonary clinics in 16 hospitals throughout Korea between June, 2005 and April, 2012. We followed the patients every three months on an outpatient basis for this cohort. Of these, the COPD patients whose lung volumes were measured at the time of enrollment were selected (n=353, Fig. 1). All patients fulfilled the following three criteria: post-bronchodilator ratio of FEV1 to forced vital capacity (FVC) <0.7 after administration of 400 µg of inhaled albuterol; more than 10 pack-years of smoking history; and no or minimal abnormality on chest radiography.
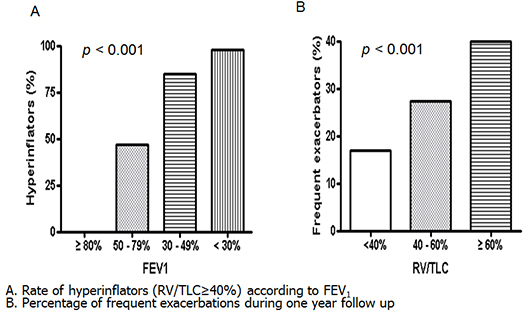
Resting pulmonary hyperinflation was defined as RV/TLC ≥ 40% (12). The patients with RV/TLC <40% served as the control group. Acute exacerbation was graded from mild to severe as previously reported after follow up for 1 yr from enrollment and only moderate and severe exacerbations were included in the exacerbation group (1314). The patients were defined as frequent exacerbators if acute exacerbation occurred twice or more per a year (1).
Clinico-physiological indices of COPD
The demographic and clinical data, including age, sex, smoking status, history of exacerbations, etc were collected.
Body mass index (BMI) was calculated as the body weight divided by the height squared (kg/m2). Dyspnea was assessed by using the Modified Medical Research Council Dyspnea Scale. Health-related quality of life was assessed by using the St. George Respiratory Questionnaire (SGRQ). Spirometry was performed by using the Vmax 22 (SensorMedics, Yorba Linda, CA, USA; PFDX instrument; MedGraphics, St. Paul, MN, USA) according to American Thoracic Society guidelines (11).
Chest computed tomography (CT) indices for COPD assessment
The chest CT indices used to assess COPD included the emphysema index, air-trapping index, and airway dimensions (15161718). To measure these indices, all patients underwent volumetric CT scans at full inspiration and expiration with a 16-MDCT scanner (the CT machines came from three manufacturers, namely, the Somatom Sensation 16, Siemens Medical Solutions, Forchheim, Germany; the GE Lightspeed Ultra, General Electric Healthcare, Milwaukee, WI; and the Philips Brilliance 16, Philips Medical Systems, Best, Netherlands) (16). The emphysema index was determined from CT data by automatic calculation of the volume fraction of the lungs below -950 Hounsfield Units at full inspiration and the mean lung density (15). The CT air-trapping index was defined as the ratio of mean lung density on expiration and inspiration (17). Airway dimensions were measured near the origin of four segmental bronchi (RB1, LB1+2, RB10, LB10) by a consensus of two radiologists using in-house software. Airway dimensions, including wall area, lumen area, and wall area percent, defined as wall area/(wall area + lumen area) ×100, were measured in each segmental bronchus (17).
Statistical analysis
SPSS version 12 (SPSS Inc., Chicago, IL, USA) was used for the analysis. All values were expressed as means±standard deviation. To compare two groups, the Chi-Square test or Fisher's exact test was used for categorical data and Student's t-test was used for continuous data. The 95% confidence intervals of each variable were calculated. A P value of less than 0.05 was deemed statistically significant. Multiple logistic regression analyses to choose significant variables in the preceding analyses were performed. The demographic variables to indicate sample profile information such as age and sex and clinically meaningful variables were included in the multiple logistic regression.
We performed cox proportional hazard regression model using coxph in library (survival) R package to account for the survival time value with possible censoring in the data. In the cox analysis, the pulmonary function test variables that correlated strongly with RV/TLC were excluded to avoid multicollinearity.
RESULTS
Baseline characteristics
The mean age of the participants was 66.7±7.4 yr and 85.6% of the cohort were male.
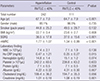
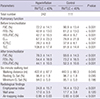
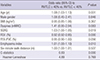
Compared to the controls, the hyperinflation group were significantly older (P<0.001) and had lower BMI (P=0.008), more severe dyspnea (P<0.001), higher high-sensitivity C-reactive protein (hsCRP) (P=0.015), lower serum albumin (P=0.007) and lower serum creatinine levels (P=0.001) (Table 1). The hyperinflation group had significantly worse quality of life (SGRQ: 36.5±17.8 vs. 27.0±15.6, P<0.001) than the controls. Pulmonary function was worse in the hyperinflation group, as measured by FEV1, FEV1/FVC, FVC, and IC/TLC (all P values<0.001) (Table 2). Moreover, the 6-min walking test distance was shorter in the hyperinflation group (P=0.045) (Table 2). However, oxygen saturation in six-minute walk test did not show significant difference between two groups (Table 2). Radiological evaluations showed that emphysema index and air-trapping index were higher in the hyperinflation group (all P values<0.001)(Table 2).
Predictors of resting pulmonary hyperinflation in COPD by logistic regression analysis
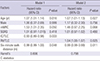
This analysis was performed to identify independent factors associated with patients with resting pulmonary hyperinflation. Multiple logistic regression analysis using the all possible risk factors in the data demonstrated that age (OR=1.08, P=0.001), SGRQ (OR=1.03, P=0.019), FEV1 (OR=0.92, P<0.001), and emphysema index (OR=1.01, P=0.010) associated independently with RV/TLC ≥40% (Table 3).
Survival analysis
The median follow-up period of all patients was 3.72 yr. Of the 37 patients with COPD who died during the observation period, death was most frequently due to respiratory failure (5 patients). Other causes were pneumonia (4 patients), acute exacerbation of COPD (3 patients) lung cancer (3 patients), cancers other than lung cancer (3 patients), myocardial infarction (3 patients), respiratory failure after surgery (2 patients), septic shock (1 patient), pneumothorax (1 patient), and suicide (1 patient). Since the cause of death was unknown in 29.7%, only all-cause mortality was used for the survival analyses.
Multivariate analysis with the Cox regression model 1 that included age, gender, MRC, SGRQ, IC/TLC, and 6-min walking distance revealed that an older age [Hazard Ratio (HR)=1.07, P=0.016)], MRC (HR=1.53, P=0.05), higher IC/TLC (HR=0.93, P=0.003), and shorter 6-min walking distance (HR=0.99, P=0.048) were independent predictors of all-cause mortality (Table 4). Multivariate analysis with the Cox regression model 2 that included age, gender, MRC, SGRQ, RV/TLC, and 6-min walking distance revealed that older age (HR=1.07, P=0.027), higher RV/TLC (HR=1.04, P=0.025), and shorter 6-min walking distance (HR=0.99, P=0.011) were independent predictors of all-cause mortality (Table 4).
The corresponding Harrell's C statistics is shown as 0.809 and 0.798 for M1 and M2 survival model at the acceptable levels, respectively.
DISCUSSION
The present study showed that older age, higher emphysema index, lower FEV1, and poor quality of life (as shown by a higher SGRQ score) were associated independently with resting pulmonary hyperinflation in COPD. This study also demonstrated that RV/TLC was an independent risk factor for all-cause mortality in COPD, although longer follow up seems to be necessary for validation.
Pulmonary hyperinflation is frequently observed in patients with COPD. Previous studies show a strong correlation between static hyperinflation and the degree of dynamic lung hyperinflation during exercise (1920212223). Recent reports also suggested that static hyperinflation as expressed by the IC/TLC ratio is an independent predictor of exercise capacity and quality of life, and moreover, the IC/TLC ratio is an independent risk factor for mortality in the COPD cohort of Casanova et al. (31224). However, a well-structured systematic analysis of RV/TLC as a prognostic factor in COPD has not been performed, to date. Therefore, this study was performed with the RV/TLC values in the KOLD cohort.
Several noteworthy findings were obtained.
First, an older age and airflow limitation were independently associated with resting pulmonary hyperinflation in COPD. It has been assumed that because emphysema progresses with age, older age can contribute to static hyperinflation. However, no epidemiological study has yet shown how much RV/TLC worsens with aging, similar to the age-related decline in FEV1. Longitudinal follow-up with lung volume measurements is required to address that question, despite our finding that older age was an independent predictor of resting pulmonary hyperinflation.
The second important finding is that the hyperinflation group associated independently with higher SGRQ score, indicating that resting pulmonary hyperinflation linked with quality of life in COPD. Quality of life is an essential tool to monitor COPD and SGRQ is a COPD-specific questionnaire to assess health related quality of life, although it is not easily used on an outpatient basis because it is time-consuming (25). Though there is a report that SGRQ score is an independent marker for mortality in patients with COPD, our study did not prove it in multi-variate analysis (26).
The third important finding is that RV/TLC and 6-min walking distance were independent risk factors of all-cause mortality in COPD. Our observation is supported by two studies which suggested that RV/TLC is a predictor of survival in COPD (67). The prospective multicenter study by Nishimura et al., reported that the COPD patients who did not survive the 5-yr observation period had a higher RV/TLC than the survivors (6). However, RV/TLC was not mentioned as an important predictor of mortality because survival analyses based on RV/TLC with Cox regression method were not performed in that study (6). The more recent study showed that RV/TLC was an independent predictor of all-cause mortality in COPD (7). However, only severe COPD was included in that study. Our study expands on these observations, because 67.7% of the present study cohort consisted of patients with mild or moderate COPD (FEV1% ≥ 50). RV/TLC still remained a significant predictor of all-cause mortality even in overall milder COPD.
It should be noted that other COPD cohorts had lower frequencies of patients with mild or moderate COPD. Such patients comprised 44.2% of the ECLIPSE study cohort and 29.8% of the cohort of Celli et al. (2728). Moreover, our cohort had milder COPD compared to the cohort of Casanova et al. (3), of which 45% had severe COPD (FEV1% 30-49) and 25% had very severe COPD (FEV1% <30): only 27.5% and 4.8% of our cohort had severe and very severe COPD, respectively. Therefore, different findings of our study compared to the other studies can be attributed to the disparity between the cohorts (32728).
However, a relative short term follow up of our study (median follow-up period=3.72 yr) can be a limitation in interpreting our survival analysis. This means that our findings cannot be generalized until they are validated by future studies.
Our data showed that 6-min walking distance was an independent risk factor for mortality in patients with COPD, though its association with RV/TLC was not proven in the multi-variate analysis. Our finding is supported by previous reports that the 6-min walking distance is a significant prognostic marker as one of the BODE index parameters in COPD (2729).
We acknowledge several limitations of this study. First, the small size of the cohort is a major limitation because COPD is a heterogenous disease with many phenotypes. Therefore, future studies are required to validate our main observations. Second, since 85.5% of patients survived the observation period, a longer follow-up period is needed to make the survival analysis more powerful. Third, the COPD assessment test score was not analyzed in our study because it was not obtained in the initial enrollment period. Fourth, we did not take into consideration the history of medication in our analysis, because this study was not a randomized controlled trial.
In conclusion, this study of the KOLD COPD cohort suggested that an older age, higher emphysema index, higher SGRQ scores, and lower FEV1 were associated independently with resting pulmonary hyperinflation measured by RV/TLC. RV/TLC is an independent risk factor for all-cause mortality in COPD, though short observation period is a limitation for interpretation.


 XML Download
XML Download