

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by airway inflammation and progressive airflow obstruction, most commonly caused by cigarette smoking. Airflow limitation is measured via the FEV1 (forced expiratory volume in the first second) and recognized symptomatically as dyspnea. Fletcher and Peto (1) reported that the degree of airflow obstruction was a predictor of mortality. FEV1 is used as the main parameter in the evaluation of many aspects of COPD (2). Dyspnea is also a useful measure of COPD, because this symptom is closely related to the patient's the quality of life. Some studies have reported that mortality increases according to the severity of dyspnea in the patients with stable COPD (345).
In addition to dyspnea, cough and phlegm are the major symptoms reported by COPD patients (6). Cough and phlegm are in fact reported as frequently as dyspnea in COPD patients (the frequency of cough, phlegm, and dyspnea have been reported as 70%, 60%, and 67%, respectively). Cough and phlegm are also important, because the presence of cough and sputum identifies patients at greater risk of subsequent exacerbation as defined by the need for antibiotics or corticosteroids (78). Although many clinical trials have revealed that dyspnea in COPD patients is improved by inhaled bronchodilators, the effect of these inhalers on cough or phlegm has rarely been evaluated. In recent years, new 24-hr, ultra-long-acting β-agonists such as indacaterol appear to have had a greater effect on inspiratory capacity, a marker of hyperinflation (910). The improvement of dyspnea symptoms was reported to be concomitant with decreased hyperinflation in one previous systematic review and meta-analysis (11). However, the effect of indacaterol on cough and phlegm was not evaluated in that report, despite almost all studies on indacaterol reporting a beneficial effect on dyspnea in COPD patients. Therefore, we aimed in our current study to investigate the effects of indacaterol on the symptoms of cough and phlegm in stable COPD patients.
MATERIALS AND METHODS
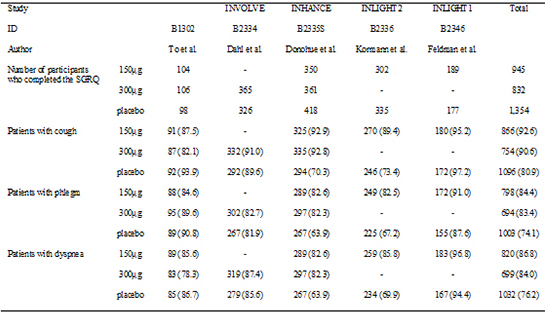
We included five randomized controlled trials (RCTs) conducted by Novartis i.e. B1302 (12), B2334 (13), B2335S (14), B2336 (15), and B2346 (16) in which 150 µg or 300 µg per day of indacaterol was compared with placebo in stable COPD patients. In our current analysis, we compared the effect of 150 µg or 300 µg per day of indacaterol with placebo according to the ratio of patients with respiratory symptom improvement after 12 weeks of treatment. We obtained the unpublished symptom scores of the St. George's Respiratory Questionnaire (SGRQ) data from the five RCTs at baseline and after 12 weeks of indacaterol treatment.
The SGRQ symptom score was zero if symptom of cough, phlegm, or dyspnea existed not at all; 1, only with lung or respiratory infections; 2, a few days a month; 3, several days a week; 4, almost every day. In our current analysis, we only included the patients who reported symptoms of cough, phlegm, or dyspnea (i.e., ≥1 of the above scores) at baseline. The improvement of symptoms denoted a lower score at 12 weeks than at baseline. We performed separate analyses for the comparison of 150 µg of indacaterol versus placebo and for 300 µg indacaterol versus placebo.
Additionally, we performed a subgroup analysis in which we excluded the patients who reported cough, sputum, or dyspnea only with lung or respiratory infections in addition to the patients who did not report symptom at all.
Statistical analysis
A relative ratio (RR) was used to evaluate treatment effects on the major symptoms - cough, phlegm, and dyspnea - comparing the indacaterol groups with the placebo group. The data were inspected to determine whether an analysis with a random effects model using the method of Der Simonianand Kacker (17), with the estimate of heterogeneity being taken from the inverse-variance fixed-effect model (18), was required. We calculated the 95% confidence intervals around the RRs. The weights as a percentage of the overall total were applied to find the interaction within each subgroup separately. Statistical heterogeneity between trials was analyzed using a chi-square test and by the I2 statistic. A test of whether the summary effect measure is equal to the null was performed, as well as a test for heterogeneity (i.e., whether the true effect in all studies is the same). Heterogeneity was also quantified using the I-squared measure (18). I2 values greater than 25%, 50%, and 75% were considered evidence of low, moderate, and high statistical heterogeneity, respectively. Meta-analyses were conducted using metan command in Stata SE 13.1 for Mac (StataCorp., College Station, TX, USA).
RESULTS
The five studies included in our analysis performed trials on 3,547 patients with COPD (Table 1). A total of 3,325 of these patients completed the SGRQ (945 patients treated with 150 µg of indacaterol and 832 patients treated with 300 µg of indacaterol). Four of 5 studies compared 150 µg of indacaterol and 3 of them compared 300 µg of indacaterol with placebo. There was no significant difference in age, sex, smoking, or baseline FEV1 between the indacaterol and placebo groups.
Indacaterol 150 µg versus placebo
At baseline, a cough (i.e., symptom score ≥1) was reported in 866 patients allocated to the 150 µg indacaterol group and 804 patients in the placebo group (Table 2). After 12 weeks of treatment, an improvement of the cough was reported in 316 (36.5%) patients in the indacaterol group and 259 (32.2%) patients in the placebo group (Relative Ratio [RR], 1.12; 95% confidence interval [CI], 0.98-1.29; P=0.066, I2=0.0%; Fig. 1A)
At baseline, phlegm was reported in 798 patients allocated to the indacaterol group and 736 patients in the placebo group (Table 2). At 12 weeks after treatment, an improvement in phlegm production was reported in 247 (31.0%) patients in the indacaterol group and 247 (30.6%) patients in the placebo group (RR, 1.01; 95% CI, 0.87-1.18; P=0.85, I2=0.0%; Fig. 1B).
At baseline, dyspnea was reported in 820 patients allocated to the indacaterol group and 753 patients in the placebo group (Table 2). After 12 weeks of treatment, an improvement of dyspnea was reported in 324 (39.5%) patients in the indacaterol group and 237 (31.5%) patients in the placebo group (RR, 1.33; 95% CI, 1.03-1.50; P=0.001, I2=55.1%; Fig. 1C).
In the subgroup of patients with symptom score ≥2 at baseline, an improvement of the cough was reported in 299 (36.6%) patients in the indacaterol group and 247 (38.4%) patients in the placebo group at 12 weeks after treatment (RR 0.95; CI, 0.74-1.22; P=0.22, I2=63.8%). An improvement in phlegm was reported in 233 (31.1%) patients in the indacaterol group and 211 (30.5%) patients in the placebo group at 12 weeks after treatment (RR, 1.03; 95% CI, 0.88-1.20; P=0.76, I2=0%). An improvement of dyspnea was reported in 370 (45.7%) patients in the indacaterol group and 246 (33.7%) patients in the placebo group (RR, 1.36; 95% CI, 1.20-1.54; P<0.001, I2=0%).
Indacaterol 300 µg versus placebo
At baseline, a cough (i.e., symptom score ≥1) was reported in 714 patients allocated to the 300 µg indacaterol group and 678 patients in the placebo group (Table 2). After 12 weeks of treatment, an improvement in cough was reported in 272 (38.1%) patients in the indacaterol group and 226 (33.3%) patients in the placebo group (RR, 1.07; 95% CI, 0.93-1.25; P=0.043, I2=25.7%; Fig. 2A).
At baseline, phlegm was reported in 694 patients allocated to the indacaterol group and 623 patients in the placebo group. After 12 weeks of treatment, an improvement in phlegm was reported in 209 (30.1%) patients in the indacaterol group and 188 (30.2%) patients in the placebo group (RR, 0.99; 95% CI, 0.84-1.18; P=0.98, I2=0%; Fig. 2B).
At baseline, dyspnea was reported in 699 patients allocated to the indacaterol group and 631 patients in the placebo group. After 12 weeks of treatment, an improvement in dyspnea was reported in 306 (43.8%) patients in the indacaterol group and 212 (33.6%) patients in the placebo group (RR, 1.29; 95% CI, 0.98-1.70; P<0.001, I2=68.3%; Fig. 2C).
In the subgroup of patients with symptom score ≥2 at baseline, an improvement of cough was reported in 258 (36.6%) patients in the indacaterol group and 212 (40.6%) patients in the placebo group (RR, 0.89; 95% CI, 0.58-1.37; P=0.083, I2=87.6%). An improvement of phlegm was reported in 196 (30.4%) patients in the indacaterol group and 172 (30.0%) patients in the placebo after 12 weeks of treatment (RR, 1.01; 95% CI, 0.85-1.20; P=0.88, I2=0.0%). An improvement of dyspnea was reported in 340 (48.8%) patients in the indacaterol group and 223 (35.1%) patients in the placebo group after 12 weeks of treatment (RR, 1.39; 95% CI, 1.13-1.70; P<0.001, I2=55.0%).
DISCUSSION
In our current review, we found that treatment with the new 24-hr, ultra-LABA indacaterol appears to have little effect on cough or phlegm in 3,325 patients with COPD. By contrast, the data show that indacaterol improved dyspnea compared with placebo. COPD is a heterogeneous disease and although chronic cough and sputum production are necessary components of the definition for COPD, changes in cough and phlegm symptoms themselves have not been well-studied. Quantifying the degree to which cough responds to treatment for COPD is difficult. Cough and phlegm in many COPD studies are just described as part of the total SGRQ score or the COPD assessment test (CAT); however, these tools are generally indicated for assessment of quality of life or health status rather than major symptoms in patients with mild to moderate lung function but with generally healthy status except cough or phlegm. Cough and phlegm does not stand out in these tools, which give a low weight to these two symptoms. Recently, newer instruments such as the EXACT questionnaires (19) were introduced. However, there is a lack of investigation of the effectiveness of these questionnaires.
A previous meta-analysis (1120) reported improvements in the symptom of breathlessness. They used a measurement involving a ratio of baseline dyspnea index (BDI)/transition dyspnea index (TDI) score. The BDI/TDI ratio considers three components-functional impairment, the magnitude of task, and the magnitude of effort-that provoke breathing difficulty. These measurements reflect the severity of patients' feelings of dyspnea. Our results showing an improvement in the SGRQ symptom domain score of dyspnea coincide with this previous meta-analysis (1120). Likewise, the improvement in the SGRQ symptom domain score of cough or phlegm could be used for the evaluation of improvement in cough or phlegm symptoms. Several studies (2122) have reported that the symptom domain score in SGRQ could be represented and associated with cough or sputum; however, how much of an improvement of symptom score of the SGRQ would be required to achieve a minimal clinical threshold of importance was unclear. Although it may be arbitrary to define a change as an improvement when one or more symptom scores within the SGRQ decrease, we should be careful to make such an interpretation. In our current study, we sought to understand the potential effect of indacaterol on cough or sputum in addition to dyspnea. However, many clinical trials on COPD have not evaluated the effects of treatment on cough or sputum per se.
Based on our current findings, the ultra-LABA which is well-known to be one of best drugs for COPD treatment did not improve cough or phlegm symptoms in COPD patients. Previous studies (2324) have reported that beta2-agonists could improve the mucocilliary function and decrease phlegm and cough symptoms. However, we did not find such an effect in our present investigation. Additionally, the effect of indacaterol on dyspnea did not show a dose-dependent correlation. Patients who were included in our current analysis had moderate to severe COPD and a mean FEV1 at approximately 50% of the normal value. The main symptoms might differ according to the FEV1 in COPD patients. Paradoxically, patients with mild to moderate COPD complain more about cough and phlegm impacts. We were not able to evaluate the effect of indacaterol on cough or sputum in a subgroup of patients with mild to moderate COPD, because we could not get access to the raw data. It is possible that our conclusions in relation to cough or phlegm may have been different if only patients with mild to moderate COPD had been evaluated. Further studies to evaluate subgroups of patients according to their lung function or other characteristics such as the frequency of exacerbation would likely be valuable.
There is a lack of COPD studies that have used cough or phlegm as outcomes per se. By contrast, the data show that indacaterol improved dyspnea compared with placebo. The effect of indacaterol on cough or phlegm has not typically been evaluated despite nearly all of the studies on indacaterol reporting a beneficial effect on dyspnea in COPD patients. We here investigated whether patients with COPD felt an improvement of symptoms such as cough, phlegm, and dyspnea after ultra LABA treatment compared to the placebo group. We conclude that compared to a placebo, a 12-week treatment of indacaterol, a long-acting beta-agonist, might not have a significant effect on cough or phlegm in stable COPD cases.



 XML Download
XML Download