

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute myeloid leukemia (AML) is the most common type of leukemia, and it has the lowest survival rate of all leukemia types in adults (1). Although attaining complete remission (CR) is the important goal of initial therapy in AML, the median disease free survival of patients who received the induction therapy only without post-remission therapy is four to eight months (23). In the past two decades, little has changed in induction chemotherapy (4). However, improved understanding of the AML biology with modern cytogenetics and molecular testing has led to the customization of post-remission therapy based on relapse risk-stratification (56). Hematopoietic stem cell transplantation (HSCT) has been considered a potentially curative therapy for AML with intermediate and adverse cytogenetics (7). However, several factors, such as old age, absence of a matched donor, and comorbidities, enable only about one-third of patients to be eligible for HSCT (8). The remaining patients who cannot receive HSCT should be followed up until disease progression after two to four courses of high-dose cytarabine-based chemotherapy and more than half of these patients eventually relapse (9). For decades, although several trials with different strategies of maintenance therapy have been conducted to reduce the relapse of disease in patients, these trials have failed to show the improvement of outcomes (10111213). Consequentially, maintenance chemotherapy is not a standard therapy for AML except for acute promyelocytic leukemia (APL).
Nonetheless, reducing the relapse rate and the prolongation of the relapse free interval by minimizing the residual disease and preventing the regrowth of dormant leukemic stem cells through the prolonged exposure to maintenance chemotherapy remain attractive (14). The maintenance therapy with low dose cytotoxic agents 6-mercaptopurine (6MP) and methotrexate (MTX) has been clinically proven beneficial to ALL (15) and APL (16). However, no study has been conducted yet to prove the clinical benefit of this therapy in AML. In this study, we retrospectively analyzed the clinical outcomes of AML patients who received oral maintenance therapy with 6MP and MTX after remission induction and consolidation therapy.
MATERIALS AND METHODS
Patients
From a single institute, 52 AML patients including those who were ineligible for HSCT (Age ≥ 65, absence of a matched donor and significant comorbidities) received at least one cycle of consolidation therapy in the first complete remission (CR1) were analyzed. Among these patients, 27 received maintenance chemotherapy and 25 did not.
Treatment
Patients received 6MP (50 mg/day, p.o.) and MTX (10 mg/week, p.o.) for two years or until disease progression. The historical control group had completed remission induction and at least one cycle of consolidation therapy. Then, the group received no specific anti-leukemic treatment.
Definitions and statistical analysis
Initial diagnosis and leukemia subtypes were recorded using the French-American-British (FAB) classification system (17). Cytogenetics were classified into 3 risk groups: favorable, t(8;21), inv(16); intermediate, normal karyotype or other numerical or structural abnormalities; unfavorable, 11q23 rearrangement, -5, del(5q), -7, del(7q), inv(3)/t(3;3)/ins(3;3). Leukemia-free survival (LFS) was calculated from the date of diagnosis to the last follow-up or first event (failure to achieve remission, demonstration of resistant leukemia, or relapse). Overall survival (OS) was defined as the time from diagnosis to death from any cause. The characteristics of the two groups were compared by the chi-square test or Fischer's exact test for categorical data and the Mann-Whitney U-test for continuous variables. LFS and OS were estimated by the Kaplan-Meier method and compared by the Log Rank and Breslow method. The Cox proportional hazard model was used in the multivariate analysis of prognostic factors. P values lower than 0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 13.0 (IBM, Armonk, NY, USA).
RESULTS
Patient and disease characteristics
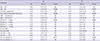
The patient and disease characteristics are given in Table 1. No significant difference was found in the baseline patient and disease characteristics between the maintenance and the historical control groups.
Treatment results
The treatment characteristics for induction, number of consolidation therapy, and cause of death are presented in Table 2. Almost all patients (96.4%) received remission induction chemotherapy with idarubicin and cytarabine. More than one-half of the patients received more than two cycles of consolidation chemotherapy. Relapse was observed in 27 patients (51.9%) who achieved CR after induction treatment. Median LFS and OS were 28 months (95% confidence interval [CI], 1-44 months) and 29 months (95% CI, 10-48 months), respectively. Disease progression (54.5%) was the main cause of death, followed by infection (34.5%). The rate of achieving CR and the number of consolidation were not statistically different between the two groups.
OS, LFS, and prognostic factors
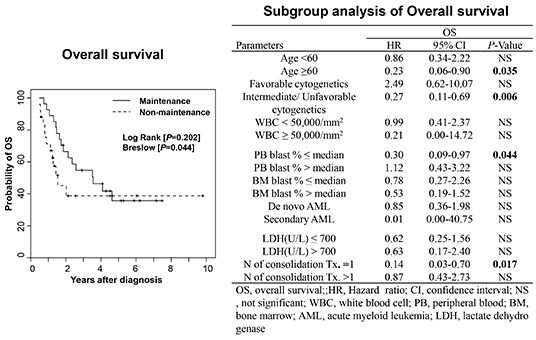
The median OS was 43 months and 19 months in the maintenance group and the historical control group, respectively (Log Rank [P=0.202], Breslow [P=0.044], Fig. 1A). The median LFS was 31 months and 12 months in the maintenance group and historical control group, respectively (Log Rank [P=0.261], Breslow [P=0.090], Fig. 1B). In the multivariate analysis (Table 3), older age was an independent poor prognostic factor for OS (P=0.020) and LFS (P=0.028). Maintenance therapy was independently associated with favorable OS (P=0.021) and LFS (P=0.024). Higher baseline WBC count was associated with shorter LFS (P=0.033).
Subgroup analysis
Subgroup analysis was performed using a univariate Cox proportional hazard model to evaluate the effects of maintenance treatment on OS and LFS (Table 4). All hazard ratios were made for patients who received maintenance treatment in comparison with those who did not. The OS (50 months vs. 16 months, P=0.004, Fig. 2A) and LFS (not reached vs. 10 months, P=0.011) were significantly prolonged with oral maintenance therapy when the cytogenetic study showed intermediate or unfavorable risk. Furthermore, clinical benefit from maintenance chemotherapy (OS and LFS) was documented for patients aged ≥60 yr (total: 17 patients, maintenance group: 11 patients, control group: 6 patients), (P=0.035, Fig. 2B and P=0.019), those with low peripheral blood (PB) blast count at diagnosis (P=0.044, Fig. 2C and P=0.022), and those who received less than two cycles of consolidation chemotherapy (P=0.017, Fig. 2D and P=0.016).
DISCUSSION
Despite intensive consolidation after achieving CR in patients with AML, less than one-third of the patients were cured, mainly because of the high incidence of relapse (18). Although several previous studies demonstrated the clinical benefit of cytarabine-based maintenance therapy (121920), these results were inconsistent (212223). However, our data indicated that oral maintenance therapy with 6MP and MTX prolonged the OS and LFS in AML patients. Moreover, the benefit was more prominent during and early after maintenance therapy.
Not all patients have experienced clinical benefit from maintenance therapy, even those with APL (242526). In one AML study, clinical benefit from maintenance therapy with tipifarnib, farnesyltransferase inhibitor was observed only in patients with secondary AML or AML with adverse cytogenetics (27). In the present study, patients with intermediate risk cytogenetics achieved more prominent OS and LFS benefits from maintenance therapy, whereas patients with favorable cytogenetics received no additional benefits from maintenance therapy. Older patients (Age ≥60), patients with low PB blast count, and patients who received insufficient consolidation therapy (≤1 cycle) obtained prominent clinical benefits from maintenance therapy. Therefore, risk-adapted maintenance therapy in AML patients may be a more appropriate approach, consistent with previous studies (2627).
As results from previous trials with conventional chemotherapy-based therapy have been regarded as negative in supporting maintenance therapy, many ongoing clinical trials have been designed with immunotherapy, demethylating therapy, or targeted therapy (14). However, it is notable that among studies using maintenance chemotherapy, those using identical consolidation regimens followed by a randomization to maintenance or no maintenance chemotherapy are rare (28). As the pharmacodynamic and pharmacokinetic features and toxicity profile of conventional agents are well known and cost effective, chemotherapeutic agents such as 6MP and MTX are good candidates for further studies about the validation of clinical efficacy as maintenance chemotherapy.
The duration of maintenance therapy is another issue. In the present study, the OS of the maintenance and non-maintenance groups was 66.5% and 45.2%, respectively, within two years, which was the period of maintenance therapy. However, five-year OS was similar between the two groups. Further studies are needed to prove that prolonged exposure to maintenance therapy is more effective and safe. Exposure to anti-cancer drugs during the two years did not evoke secondary malignancy in our result.
To our knowledge, this study is the first report about the clinical outcome of oral maintenance chemotherapy with 6MP and MTX in AML patients. However, the present study has several limitations. First, although patients were well balanced for age, cytogenetics, and prevalence of secondary AML, this study is a retrospective non-randomized study from a single institution. Second, although AML with normal karyotype is a heterogeneous group according to molecular alteration (5), AML with normal karyotype was simply classified and analyzed as an intermediate risk group, as measuring such molecular abnormalities was not routine practice throughout the duration of the study.
In conclusion, oral maintenance therapy prolonged the median OS (43 months vs. 19 months) in AML patients. Given that most AML patients in CR after several cycles of consolidation therapy experience relapse, the clinical efficacy of maintenance therapy to reduce the relapse from dormant leukemic cells needs to be reconsidered and verified by prospective randomized trials. Nonetheless, the present study suggests that AML patients, especially older patients (≥60 yr), those with intermediate or unfavorable cytogenetic results, those with initially low PB blast count (%, ≤median), and those receiving less than two cycles of consolidation therapy, could benefit from maintenance therapy with 6MP and MTX without incurring clinically or biologically significant adverse events.


 XML Download
XML Download