

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coal workers' pneumoconiosis (CWP) is characterized by a progressive fibrotic lung disease. Dust inhalation can cause a variety of lung diseases such as CWP, chronic alveolitis, and emphysema (1). CWP, a fibrotic lung disease, is characterized by a chronic inflammatory reaction associated with activation of macrophage and endothelial cells in the lung (2). Fibrosis is a disorder characterized by an alteration of the deposition of extracellular matrix with accumulation of mesenchymal cells in replacement of normal tissue (1). This pathology is usually divided into two groups: simple pneumoconiosis (SP) in which the fibrotic and inflammatory reactions remain limited, and progressive massive fibrosis (PMF) which is characterized by an extensive fibrotic reaction in the lung (3). The clinical detection of CWP, however, is currently dependent on chest radiographs.
During the past decades, it was strongly suggested that reactive oxygen species and cytokines may play important roles in coal dust exposure and related lung diseases. However, the exact consequences of the mechanisms that occur in the lungs of subjects chronically exposed to coal dust are still much a puzzle. The recruitment and adhesion of inflammatory cells including neutrophils and monocytes play an important role in lung inflammation (1). Interleukin-8 (IL-8) (4) and macrophage inflammatory protein-1α (MIP-α) (5) have been characterized as potent factors in the recruitment of inflammatory cells. Silica, one of the ingredients of coal, results in increased intercellular adhesion molecule-1 (ICAM-1) levels in the lung tissue, and was followed by a marked neutrophil influx to the lung (6). Increased ICAM-1 expression has been demonstrated in the lungs of coal miners, particularly in endothelial cells, in epithelium, and in association with alveolar macrophages (2).
Evidence from various studies in macrophages and fibroblasts suggests that there is increased production of these cytokines following exposure to crystalline silica or coal dust. However, only a limited number of validation studies have been reported in human studies (1, 8). These reports suggest the importance of serum cytokines in CWP, however there are not many reports about the in vivo relevance of the utility of predictive discrimination using the levels of cytokines to assess the fibrotic progression such as PMF.
In this study, we examined the relationship between CWP findings and the serum levels of IL-8, MIP-1α, and ICAM-1 in retired coal workers.
MATERIALS AND METHODS
Study subjects
A group of 130 male retired coal workers were recruited and examined for pneumoconiosis over two months at an affiliated hospital of the Korea Workers' Compensation & Welfare Service (KCOMWEL). We excluded 24 subjects who showed serum levels greater than criteria level for liver or kidney dysfunction indices, including aspartate aminotransferase, alanine aminotransferase, or gamma-glutamyl transpeptidase, blood urea nitrogen, or creatinine. The diagnosis of CWP was based on the changes observed on chest radiographs according to the rules of classification used by the International Labour Organization (ILO) (8). Classifications of radiographs were determined using the guidelines of the pneumoconiosis review committee of KCOMWEL in Korea. Briefly, radiographs were obtained after a consensus of classification was acquired between two experienced radiologists. The subjects were put into three groups according to the radiography classifications, so that classifications of 0/0 were placed in the non-CWP group (n=27), classifications 1/0-3/2 with small opacities were placed in the simple pneumoconiosis group (SP, n=59), and categories A, B, C with large opacities were placed in the complicated CWP, i.e. PMF, group (n=20).
Pulmonary function was measured in accordance with the guidelines recommended by the ATS/ERS task force (9) using a Vmax22 spirometer (SensorMedics, San Diego, CA, USA). The parameters measured included FVC (the volume delivered during an expiration made as forcefully and completely as possible starting from full inspiration), FEV1 (the volume delivered during the first second of an FVC maneuver), and the FEV1/FVC (%FEV1/FVC) ratio. The predicted FVC and FEV1 volumes were calculated using a previously reported equation (10). Personal information, including age, body mass index (BMI), and demographic information, were obtained using a questionnaire.
Measurement of serum cytokines
Serum levels of IL-8, MIP-1α, and ICAM-1 were measured using a bead laser analyzer (Bio-Plex 200, Bio-Rad Laboratories, CA, USA) in accordance with the manufacturer's recommendation.
Statistical analyses
Levels of serum MIP-1α were normally distributed and those of serum IL-8 and ICAM-1 were log-normally distributed. We analyzed data using one-way analysis of variance (ANOVA) followed by Tukey's comparison to identify differences between the study groups. Values of P<0.05 were considered statistically significant. All statistical evaluations were performed using SPSS 17.0 software (SPSS, Chicago, IL, USA).
RESULTS
Study subjects
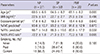
The general characteristics of the study subjects are shown in Table 1. General characteristics, including median BMI, exposure period, pulmonary function (%FVC predicted, %FEV1 predicted), and smoking status were not different between the study groups. Two characteristics were different in the study groups, age and %FEV1/FVC ratio.
Serum cytokine levels
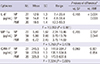
The mean level of ICAM-1 was significantly different based on smoking status (P=0.049). There were no significant differences in the levels of IL-8 and MIP-1α in serum that were associated with general characteristics such as age, exposure period, or smoking status. Furthermore, there were no significant differences in the levels of measured cytokines in serum that were associated with the criteria of predicted %FVC (80%), predicted %FEV1 (80%) or %FEV1/FVC ratio (70%) (Table 2).
Serum cytokine levels stratified by CWP diagnosis are shown in Table 3. The mean level of IL-8 in subjects with PMF (19.5 pg/mL) was significantly higher than those in subjects with NP (12.9 pg/mL, P<0.001) and with SP (14.8 pg/mL, P=0.003). The mean level of ICAM-1 in subjects with PMF (325.8 ng/mL) was significantly higher than that in subjects with NP (245.5 ng/mL, P=0.001). Although the mean level of ICAM-1 was not significantly different in these groups, the mean ICAM-1 level of subjects with SP tended to be higher than that of subjects without pneumoconiosis (279.8 ng/mL vs. 245.5 ng/mL, P=0.069), and the mean level in subjects with PMF tended to be higher than that of subjects with SP (325.8 ng/mL vs. 279.8 ng/mL, P=0.054). The mean levels of MIP-1α did not show differences among the study groups.
In the subjects without PMF, the mean level of IL-8 in subjects with ILO category II or III was significantly higher than those in subjects with ILO category 0 (P=0.006) and with ILO category I (P=0.026). The mean level of MIP-1α in subjects with ILO category II or III was significantly higher than those in subjects with ILO category I (P=0.031). Although mean level of ICAM-1 did not show significant differences among the subjects stratified by ILO category, the mean ICAM-1 level of ILO category II or III subjects tended to be higher than that of ILO category 0 (P=0.050) (Fig. 1).
DISCUSSION
CWP is characterized by chronic inflammation of the lung associated with activation of macrophages and endothelial cells in the lung (2). Toxicity and interactions of crystalline silica and coal dust in the lung are based on the activation of macrophages and lung inflammation; so many researchers have been concerned about the cytokines crucial for the pulmonary disorder resulting from exposure to these mineral dusts (1). It is important that research on potential and prospective biomarkers for pneumoconiosis should be carried out before irreversible radiological changes in the lung (11). Pulmonary fibrosis is an irreversible accumulation of connective tissue in the interstitium of the lung. Research on animal models and studies of human lung disease suggest that the initiating events may be a combination of pulmonary injury and the recruitment of inflammatory cells (12). Recruitment of inflammatory cells such as monocytes, macrophages, and neutrophils play an important role in inflammatory processes in the lung. Inflammation and its progression may depend upon dust concentration and it is proceeded even after the discontinuation of exposure (13).
Serum cytokines are increased in various liver diseases in response to alcohol (14) and the hepatitis virus (15). Serum levels of many inflammatory cytokines may be elevated in these conditions (16). Therefore, we excluded subjects who had serum levels of indicators of liver-kidney dysfunction that were greater than reference values.
IL-8 is an important activator and chemoattractant for neutrophils. The accumulation of inflammatory leukocytes in the lung is a hallmark of pulmonary inflammation (17). IL-8 is an important chemokine in the lung inflammation induced by crystalline silica (18). Levels of IL-8 were reportedly elevated in the supernatants of spontaneous or dust-stimulated monocytes (19). We previously found that serum levels of IL-8 were related to CWP (7). In this study, the mean level of IL-8 was significantly higher in PMF subjects compared to in NP subjects (P<0.001) or SP subjects (P=0.003). In the subjects without PMF, the mean level of IL-8 in subjects with ILO category II or III was significantly higher than in subjects with ILO category 0 (P=0.006) or with ILO category I (P=0.026). These results suggest that serum IL-8 level could serve as a biomarker for the presence of CWP and for progressive fibrosis in pneumoconiosis.
Initiation and propagation of CWP were dependent upon the ability of inflammatory cells to adhere to vascular walls and to migrate across the endothelium. After stimulation by inflammatory mediators, endothelial cells are able to express leukocyte adhesion molecules such as ICAM-1 (20, 21). Other cell types including epithelial cells, fibroblasts, and macrophages in lung tissue are able to express these molecules and are involved in the inflammatory process (22). Wang et al. (23) reported that the expression of ICAM-1 in sputum cells was significantly increased in patients with pneumoconiosis, and this may be meaningful for the early detection of coal pneumoconiosis. In the present study, the mean level of ICAM-1 in subjects with PMF was significantly higher than in subjects with NP (P=0.001). Although mean levels of ICAM-1 were not significantly different, the mean ICAM-1 level of subjects with SP tended to higher than subjects without pneumoconiosis (P=0.069), and the mean level of subjects with PMF tended to be higher than subjects with SP (P=0.054). These results suggest that serum ICAM-1 level could serve as a biomarker for the presence of CWP and progressive fibrosis in pneumoconiosis.
Silica particles caused a marked increase in the expression and production of MIP-1α and MIP-2. Particles have also been shown to increase proteins that comprise potent recruitment factors for neutrophils (24). Recently, MIP-1α was shown to play a role in the development and progression of silicosis inflammation (25). Although evidence was obtained from a various studies for the increased expression of MIP-1α following inflammation in the lung, only a limited number of human validation studies have been reported in the literature. In the present study, the mean level of MIP-1α was not significantly different among the study groups. However, the mean level of MIP-1α in subjects with ILO category II or III was significantly higher than in subjects with ILO category I, or in the subjects without PMF (P=0.031). Therefore, future studies should attempt to ascertain the correlation between MIP-1α levels and CWP from a larger number of study subjects.
The study has several limitations. It did not consider progressive pneumoconiosis using a longitudinal study. There is also a lack of data on co-factors like neurotrophic factor (co-factor for IL-8) (26). Although, serum levels of IL-8 and ICAM-1 tended to increase in association with the presence of CWP and PMF, IL-8 and ICAM-1 in serum are not specific biomarkers for PMF. Therefore, they are not good candidate markers for early detection of PMF. This study's implication should be limited to the association for validating mechanism of developing PMF.
In conclusion, high serum levels of IL-8 and ICAM-1 are associated with the presence of CWP and PMF. Future studies will be needed to ascertain the cytokine profiles in longitudinal follow-up studies.


 XML Download
XML Download