

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The clinical manifestations of acute myocarditis vary from asymptomatic changes in an electrocardiogram to fulminant heart failure with life-threatening arrhythmia. Fulminant myocarditis may be considered a kind of acute myocarditis due to various causes and pathogenic processes. Because the diagnosis is neither etiological nor histopathological, the clinical manifestations of cardiac inflammation with acute heart failure and severe hemodynamic compromise have been diagnostic keys. Not only medical treatment of heart failure or arrhythmia but also hemodynamic support with extracorporeal membrane oxygenation (ECMO), intraaortic balloon pumps, or ventricular assist devices (VAD), have been reported as beneficial bridges to recovery (123). The long-term outcome of children with fulminant lymphocytic myocarditis seems good if they can be supported through the acute phase, though some require transplantation (34). We report on a fulminant myocarditis patient presenting shock mimicking acute coronary syndrome, finally bridging to orthotopic heart transplantation; the pathological substratum revealed diffuse lymphocytic infiltration and myocyte necrosis in the all four cardiac chambers.
CASE DESCRIPTION
A 23-yr-old woman with no prior medical history was transferred to our emergency department in shock on December 9th 2013. Three days earlier she had a feeling of having a common cold, general weakness, and epigastric discomfort; immediately before presentation, a sudden dyspnea developed after intravenous fluid therapy on the suspicion of gastroenteritis in the local clinic. At the time of presentation, her blood pressure was 61/40 mmHg, heart rate 50 beats per minute, respiratory rate 20 breaths per minute, and body temperature 36.9℃. She looked acutely ill, and there were inspiratory crackles and coarse breathing sounds in the whole lung field.
The initial electrocardiogram showed a 2:1 atrioventricular block with ST segment elevation at V1-2 (Fig. 1A). Her chest X-ray showed pulmonary edema. Laboratory data was significant for elevated cardiac troponin I at 10 ng/mL, BNP at 459 pg/mL, creatinine at 2.33 mg/dL, and AST/ALT at 1,440/1,174 IU/L. Subsequent emergency coronary angiography revealed normal coronary arteries. The portable echocardiogram showed global hypokinesis with a left ventricular (LV) ejection fraction of 15% (LV end-diastolic dimension of 47 mm, end-systolic dimension of 44 mm, and wall thickness of 8-9 mm). Under the clinical diagnosis of acute fulminant myocarditis she was admitted to the medical intensive care unit.
Intravenous positive inotropes (dopamine, dobutamine) and amiodarone were applied due to hemodynamic instability and ongoing sustained ventricular tachycardia (Fig. 1B). Her blood pressure was 75/53 mmHg. She was conscious and tachypneic, with an oxygen saturation of 88% despite the oxygen face mask with reservoir bag and a 10 L/min flow rate. Due to the severe pulmonary edema with failure to oxygenate, subsequent rapid-sequence endotracheal intubation and mechanical ventilatory care were planned. Early after administration of weight-based doses of an etomidate and endotracheal intubation, there was a prolonged cardiac arrest and intensive cardio-pulmonary resuscitation (CPR) (total 55 min) with immediate veno-arterial ECMO support leading to successful resuscitation. Laboratory data for polymerase chain reaction (PCR) was negative in cytomegalovirus (CMV) IgM, Epstein-Barr virus (EBV) VCA or EA IgM, Adenovirus PCR, Influenza A or B virus PCR, Parvovirus B19 PCR, etc.
On the 4th day of ECMO support, the patient was alert enough to recognize her family members and obey simple commands, but the arterial pulsation curve completely disappeared. Another echocardiogram showed an increase of LV cavity dimensions without any effective contraction, with severe spontaneous echo-contrast in the LV cavity, and borderline thickened LV walls (11 mm). It also presented a lower voltage with a persistent complete atrioventricular block (Fig. 1C, D). Laboratory data revealed elevated cardiac troponin I (≥22.78 ng/mL), CK-MB at 38.7 ng/mL, and AST/ALT at 1,596/967 IU/L, with a progressive thrombocytopenia despite platelet transfusions. The patient was registered as an orthotopic heart transplantation candidate with blood type B+ and KONOS status 0.
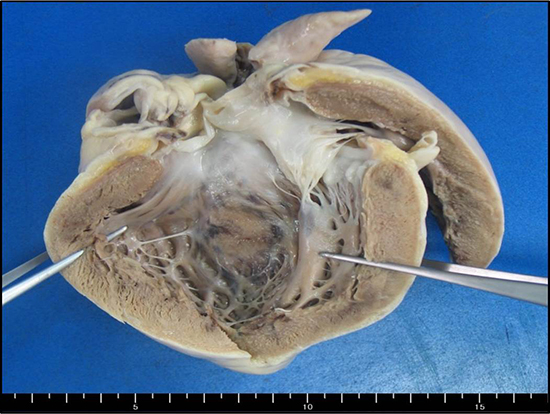
On the 5th day of ECMO, she successfully underwent orthotopic heart transplantation. A gross examination of the explanted heart showed multiple petechiae or bruises on the epicardium and necrotic spots on the endocardium (Fig. 2). Histologic findings reveal numerous foci of lymphocytic inflammatory cells and necrotic myocytes in the atrial and ventricular walls which were compatible with fulminant lymphocytic myocarditis of Dallas criteria (5) (Fig. 3). The left ventricular wall showed focal caseous necrosis and hemorrhage. There was a mild degree of endomyocardial fibroelastosis and myocardial interstitial fibrosis but no evidence of ischemic damage. To find the pathogen, PCR and immunohistochemical stain analysis were performed. PCR for CMV DNA, EBV, Pneumocystis jirovecii, and Herpes simplex virus type 1 and 2 DNA as well as the immunohistochemical strain of CMV, EBV, Adenovirus, BK virus, and Pneumocystis jirovecii, were all negative.
The immediate after-transplantation period was complicated with acute renal failure and pneumonia requiring intermittent hemodialysis or continuous renal replacement therapy and intravenous antibiotics. ECMO weaning was successful on post-operative day 2. The acute renal failure was completely resolved after a few weeks. The routine one year following work-up revealed no evidence of acute cellular rejection (Grade 0 R, AMR 0) and normal LV systolic function.
DISCUSSION
Fulminant myocarditis is a rare clinical syndrome of all types of myocarditis, presenting acute heart failure and severe hemodynamic compromise requiring pharmacological or mechanical support. The prevalence was reported as 11% in biopsy-proven myocarditis (6), with a higher incidence in children or young adults (7) who were previously healthy.
With an abrupt circulatory collapse there is a rapid diagnostic challenge for fulminant myocarditis. In this case, in the setting of cardiogenic shock with high cardiac troponin I and ST segment elevation, acute myocardial infarction should be ruled out. Among the cardiac imaging studies, portable echocardiography seems essential to evaluate initial suspicions of fulminant myocarditis; other modalities such as cardiac MRI can be more promising in principle to evaluate an inflamed myocardium (8) but are often limited in real clinical practice due to the patients' hemodynamic instability or the requirement for mechanical support devices. Portable echocardiography is also helpful to give an immediate report of the myocardial functional recovery status (the LV dimension and function), to detect complications (thrombus, pericardial effusion), and to understand flow hemodynamics (aortic regurgitation, or formation of mixing cloud along the aorta), especially in patients with ECMO support.
The underlying etiologies of the acute fulminant myocardial inflammatory process are various - viral, bacterial, toxic, or even autoreactive. The prevalence of cardiotropic viruses in endomyocardial biopsies in inflammatory myocarditis also varies widely: enterovirus in 3% to 53%, CMV DNA in 3% to 40%, and adenoviruses in 3% to 23% of the patients (9). It is important to have histopathologic findings to treat rare but specific cases of fulminant myocarditis, such as giant cell myocarditis, cardiac sarcoidosis, or eosinophilic heart disease (10). In this case, an initial endomyocardial biopsy was missing due to prolonged CPR and ECMO support; however, a blood test with PCR and all ancillary studies from the explanted heart failed to reveal any specific etiology or pathogen. Hence, the treatment strategies could not have been pathogen-specific, being based instead on aggressive heart failure and anti-arrhythmic management with early utilization of mechanical circulatory support.
Favorable outcomes have been reported using either ECMO or VAD (LV or Biventricular) (1231112). The generically best option is not clear, but if the duration is shorter, ECMO may be better since it is easier to wean the patient off of it; for a longer period, biventricular VAD seems reasonable. In Korea, a VAD is not typically available, resulting in a default choice for ECMO. In one registry of 514 pediatric patients with myocarditis, ECMO was applied in 18.9%, VAD in 4.3%, both ECMO and VAD in 2.9%, and heart transplantation in 4.1% (4).
The optimal criteria for heart transplantation in patients with fulminant myocarditis on ECMO are not universally agreed upon. Although results of ECMO are excellent (23), prolonged support is associated with significant morbidity such as peripheral vascular, hemolytic, or thromboembolic complications. The bridge to transplantation is crossed if there is not sufficient myocardial functional recovery within the limited, tolerable ECMO period. Fulminant myocarditis, although a serious illness, may be more likely to lead to full recovery than other types of acute myocarditis (6), often within 2 weeks (13), and recurrent myocarditis has also been reported in the transplanted heart (14). We authors think heart transplantation should be the very last option for patients who fail to recover despite mechanical support.
Deciding that there is no hope for myocardial recovery with impending clinical death and so deciding to replace the heart is still clinically challenging, especially in oriental cultures with a relative lack of heart transplantation donors. In particular, if the decision is too late, it may take too long to have the next available cardiac donor - weeks to months. In this case, there was no critical hemolytic or thromboembolic complication, but the daily troponin I level was not decreased and there was progressive thrombocytopenia despite several transfusions. Although not conclusive, the electrocardiographic changes were significant, from sustained ventricular tachycardia to a complete atrioventricular block, and the loss of the R-wave which may reflect a lack of myocardial recovery (15). The daily echocardiograms revealed no contractile improvement of the LV myocardium. All these led to a subsequent bridge to orthotopic heart transplantation.
In addition to ECMO support, we considered other procedures such as cardiac decompression via additional LV cannulation or atrial septostomy (16). Even though her non-contractile LV cavity stepwise increased with profound spontaneous echo-contrast, the actual measured LV dimension was still in the normal range - the stasis seemed to arise mainly from a lack of LV movement rather than significantly elevated end-diastolic pressure. After watching very closely, we ultimately decided not to use additional venting.
To our knowledge this is the first case to show the gross pathologic features of both ventricles in fulminant lymphocytic myocarditis. It was fascinating to see the diseased heart in vitro and to do the PCR and immunohistochemical stain to find pathogens in the heart. The size and weight of the explanted heart was normal in an ethnic context (17). The external surface petechiae-like lesions might have come from the prolonged CPR. On gross inspection, endomyocardial mottled changes were more prominent in the left than the right ventricle, but the microscopic evaluation of the right ventricular wall revealed numerous lymphocytic infiltrations. The right heart involvement in myocarditis is reported at over 70% (13). All four cardiac chamber walls showed lymphocytic infiltration and myocyte necrosis fitting the Dallas histopathological criteria (5) of fulminant myocarditis.
In summary, fulminant myocarditis is well known but still involves both diagnostic and therapeutic challenges, the condition sometimes leads suddenly to a critical circulatory collapse that requires immediate, aggressive, and prolonged mechanical-device support to bridge to recovery, or even to transplantation. The physician needs to ensure the spontaneous availability of that support for such patients



 XML Download
XML Download