

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Surgical closure has been the gold standard for the treatment of adult patients with atrial septal defect (ASD) (1). Since the first attempt of transcatheter device closure of ASD in 1970s, however, it has become an effective alternative therapy to surgical repair in patients with single ASD of secundum type (23). As the improvement of devices, percutaneous closure of ASD with multiple defects has also been attempted and closed successfully (45).
Although percutaneous device closure of ASD is known to be safe, several potential complications may develop (678). Embolization of the occlusion device after percutaneous closure of ASD is one of the most disastrous complication even though it is rare. The usual site of embolization is the right side of the heart including pulmonary artery, but the device embolization to the extracardiac aorta is an extremely rare complication (8). Embolization of Amplatzer Septal Occluder (ASO) to the ascending aorta, aortic arch, or abdominal aorta in a patient with single ASD has been described so far (8).
Here, we report a successful percutaneous retrieval case of the embolized ASO to the descending thoracic aorta after the successful deployment of two ASO devices in a patient with double ASD with review of the literature.
CASE DESCRIPTION
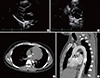
A 27-yr-old male presented with mild dyspnea. Physical examinations were non-specific except for the fixed splitting of second heart sound on auscultation. Electrocardiography showed normal sinus rhythm with right atrial enlargement and right bundle branch block. Transthoracic (TTE) and transesophageal echocardiography (TEE) revealed dilated right ventricle and atrium (Fig. 1A), abnormal left to right shunt flow through maximally 10.1 mm (superior rim) and 14.3 mm (inferior rim)-sized two ASDs of secundum type (Fig. 1B), and the calculated ratio of pulmonary (Qp) to systemic blood flow (Qs) was 1.8. Around superior defect showed the 9.3 mm sized-aortic rim, and another defect was seen inferiorly with 8.2 mm-sized intervening septum between them. Postero-inferior rim was measured as 13.6 mm, and no defect was shown posterior to the superior one with 29 mm-sized floppy posterior rim. Under the TEE and fluoroscopic guidance, percutaneous device closure of double ASD was performed using ASO. Balloon-sizing diameter of each ASD was measured as 13.5 mm and 15 mm using stop-flow technique, and thereby 14 mm- and 16 mm-sized ASOs were placed in each defect in order and deployed one by one subsequently and successfully (Fig. 1C). Final TEE revealed good apposition of two ASO devices with minimal residual shunt flow (Fig. 1D).
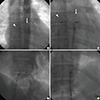
The patient experienced sudden and transient chest discomfort on the next day. On the third day, pre-discharge follow up TTE was showed no visualization of one of the deployed ASO devices, which was located in postero-inferior rim (Fig. 1D), with de novo left to right shunt (Fig. 1E), and the other ASO showed stable position. The embolized ASO was identified in the descending thoracic aorta on careful TTE examination and chest CT angiography (Fig. 2). Because TTE showed decreased amounts of shunt through the remained ASD with decreased size of the right ventricle, percutaneous retrieval of the embolized ASO was planned without performing ASD closure. After 10-french catheter was introduced through the femoral artery, the embolized ASO was successfully retrieved by snaring the screw on the right atrial disc of ASO (Fig. 3). The patient have not had any symptoms and events for 1 yr of clinical follow up.
DISCUSSION
As the percutaneous transcatheter device closure has been accepted and widely used for the treatment of ASD, several device related safety issues or unexpected complications such as atrial perforation, thrombus formation, hemopericardium associated with erosion of aorta, device embolization have also been described (678). Embolization of the occlusion device after percutaneous closure of ASD is one of the most disastrous complication even though it is rare (8). The incidence of device embolization after device closure of ASD is varied from 0.01% to 0.55% (89). In a recent study of 284 cases of ASD device closure, device embolization was reported up to 1.4% (10). In the present case, ASO was embolized to the descending thoracic aorta. According to the previous study, the usual site of embolization is the right side of the heart including pulmonary artery, but the device embolization to the extracardiac aorta, as shown in the present case, is very rare (9).
Device embolization after percutaneous ASD closure usually developed during the procedure or immediate peri-procedural period (8910), but late embolization has been described also (1112). Considering clinical symptoms of the patient, device embolization might be developed at the second hospital day and identified at the third hospital day after successful ASD closure in the present case.
Device embolization was treated by percutaneous retrieval by using gooseneck snare in the present case. In the early period of transcatheter occlusion of ASD, device embolization is usually treated by surgery (101112), but more recently it is usually treated by percutaneously by using snares or biopsy forceps (9131415). Therefore, it would be a reasonable therapeutic strategy to try percutaneous retrieval of the embolized device initially before performing surgical removal.
The proposed mechanism or predisposing conditions of device embolization are as follows; undersized device, inadequate or floppy rim, and operator-related technical issues such as poor experience or device malposition or excessive tension (816). However, these predisposing risk factors for device embolization were not identified, and thus other risk factors might be involved in the present case (Fig. 4). The authors suggested that competitive movement between the two devices to obtain their stable positions, especially in the overlapped site of the devices, would be a possible explanation of the device embolization in the present case.
Percutaneous treatment strategy of multiple ASDs has been constantly evolving. Mehta et al. (17) studied in 28 patients with multiple ASD and found that the ability of the Helex Septal Occluder (HSO) devices to overlap or sandwich each other may make it an ideal choice particularly when multiple devices need to be implanted. Song et al. (18) reported that 2 occluders are necessary for the distance of two ASDs more than 7 mm, but a single occluder is sufficient for those 7 mm and less. Since the intervening septum between two defects was measured as 8.2 mm, it would be appropriate to choose two-device closure in the present case. However, interventional cardiologist who undergoes device closure for ASD with multiple defects should keep in mind and closely monitor the possibility of late device embolization even though initial transcatheter closures of ASDs are successful. To the best of our knowledge, the present case was the first report on the late embolization of one Amplatzer device after the successful deployment of 2 ASO devices for double ASDs. Considering the present case, multiple ASDs or implantation of multiple devices should be added as one of the important risk factors for device embolization.


 XML Download
XML Download