

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Psychological stress after trauma has long been recognized as an important factor in the development of mental disorders (1). Childhood traumatic events, such as child abuse, parental death, bulling by peers, natural disasters, and medically related trauma, are associated with various negative mental health outcomes. These include anxiety, depression, substance abuse, posttraumatic stress, dissociation, oppositional behavior, suicidal and self-injurious behavior, anger and aggression, risk-taking behavior, and age-inappropriate sexual behavior (2345).
Among various types of adverse childhood experiences, child sexual abuse has been remarkable academic and public issues in Korea. A child sexual abuse response team, the Sunflower Center was established at Yonsei University Health System by the Ministry of Gender Equality and Family of Government in 2004. Currently there are 34 Sunflower Center are operating in Korea, and over 5,000 sexually abused children under the age of 13 are being serviced every year. The need to evaluate sexually abused child victims has been growing and the standardized, normed tests of trauma-related symptoms in children has been lack and not available to Korean clinicians.
Thorough and accurate assessment is requisite for the implementation of appropriate interventions for children and adolescents after traumatic events (7). Several trauma symptom measures have been translated into Korean. The children's revised impact of Event scale (CRIES) and Clinician-Administered PTSD Scale for Children and Adolescents (CAPS-CA) are most commonly used ones (89). However, non-inclusion of the hyperarousal dimension in the IES and the time involved in administering the CAPS-CA make it difficult to use as a screening tool in normal clinical settings (810). The Davidson Trauma Scale (DTS) is a reliable and valid tool for assessing trauma symptom and a self-rated assessment that requires a very short amount of time to complete, but it had been studied only in adult subjects in Korea (11). For these reasons, development of the Korean version of useful scale is necessary to evaluate children and adolescents with trauma, especially younger sexual abuse victims.
Among currently available measures for use by clinicians and researchers, we need the instrument that can screen PTSD as well as the multiple symptoms of trauma such as depression, anger, sexual concerns. It also should have the proven norms and data on clinical psychometrics, and be user-friendly regarding time needed to administer and the appropriate age group of the child for clinical purpose (7). As regarding the criterion of user-friendliness and time to administer, the self-report measures are favored because they take a shorter time to administer than clinician-administered interview format. In the self-report measures, there are client self-reports and parent-self reports (7). Concerning criteria for age in a Sunflower center, sexually abused children under age 13 had been the target group to evaluate and treat by the government at first because of the limitation of development of cognitive and communicative development.
Among various measures satisfying these criteria, there are the Trauma Symptom Checklist for Children (TSCC) and the Trauma Symptom Checklist for Young Children (TSCYC) (7121314). The TSCC is a self-report instrument made to recognize a broad range of symptoms of childhood traumatic experiences in 8 to 17 yr old children and adolescents (71415). This 54-item questionnaire takes approximately 10 to 20 min to complete. The Korean version of the TSCC is a screening instrument with satisfactory psychometric qualities and it is capable of identifying self-reported experiencing trauma symptoms among children and adolescents who have experienced trauma (15). The TSCC is designed for the child older than 8 yr because younger children may not be able to fully understand what a given psychological symptoms or internal state actually represents because of insufficient cognitive development, or not be able to comprehend written test items well enough for responding properly (12).
The TSCYC is 90-item caretaker report measure and takes 10 to 20 min to complete in the caretakers of children and adolescents aged from 3 to 12 (1213). Both scales measure post traumatic symptoms, PTSD symptom cluster and abuse related symptoms associated with trauma in children including sexual assaults. However, the TSCYC would be more appropriate to use for the younger children, especially preschoolers who have insufficient cognitive development for self-report (12). Moreover, the TSCYC includes specific scales to verify the validity of caretaker reports unlike most other parent/caretaker-report measures. Therefore, the purpose of our study was to develop a Korean version of the TSCYC and to evaluate its reliability and validity in normative and traumatized samples with child sexual abuse in a Korean population of children and adolescents.
MATERIALS AND METHODS
Participants
Normative group
A total of 307 children's caretakers agreed to participate in the study and rated the behavior and symptoms of their children. The caretakers rated children 3 to 12 yr old, who were attending one kindergarten and one elementary school in Daegu, which is the fourth largest city in Korea with approximately 2.5 million inhabitants. Permission was obtained in advance from the headmasters and teacher and parents' committee of the school board of the school in which the study was performed. All the participants, their caretakers and school students, had given the informed consents. The ethics committee of Kyungpook National University Hospital granted permission for the study. We excluded the participants with prior psychiatric diagnosis and treatment. Also, eight were excluded because of missing data, and the final sample included 299 subjects; 137 boys and 162 girls. The mean age in the normative group was 7.51 yr old (SD=2.75); boys only, 7.34 (SD=2.80) and girls only, 7.68 (SD=2.86).
For the purpose of test-retest reliability, 88 students were randomly selected, and their caregivers completed the TSCYC a second time, 4 weeks later.
Traumatized group
The traumatized group consisted of 73 abused children (51 girls and 22 boys) who consecutively visited the Sunflower Center, treatment center for sexually abused children in Deagu. Parents or other caretakers and children gave informed consent to participate. All clinical cases had been sexually abused (corroborated by police reports and medical charts). The age in the traumatized group varied between 3 and 12 yr (boys, mean age 9.14, SD=2.17; girls, mean age 7.66, SD=2.70). The TSCYC was completed before the start of the treatment, and no psychiatric diagnoses were made at that time.
The mean age for total sample and each gender group were not significantly different between normative and traumatized groups. In the normative group, fathers and mothers had significantly more years of education (t=1.09, P<0.001, t=1.60, P<0.001) than those in the traumatized group. In the normative group, 92.3% of children had been living with their both parents, which was significantly higher proportion (χ2=11.71, P< 0.001) than 42.5% in the traumatized group. Socioeconomic status of the normative group had been significantly higher than in the traumatized group (χ2=2.72, P<0.001) (Table 1).
Questionnaires
Trauma symptom checklist for young children
The TSCYC is a 90-item caretaker-report instrument, developed for the assessment of trauma-related symptoms in children aged 3-12. Items are rated on a 1 ("not at all") to 4 ("very often") scale. The scales of the TSCYC include two caretaker report validity scales, Response Level (RL) and Atypical Response (ATR). The Response Level validity scale assesses potential under-report which taps a general tendency to deny normal, minor problematic behavior in one's child. The Atypical Response validity scale assesses potential over-report which evaluates parent/caretaker willingness to endorse a series of very unusual and unrelated behaviors. The questionnaire includes nine clinical scales: Posttraumatic Stress-Intrusion (PTS-I), Posttraumatic Stress-Avoidance (PTS-AV), Posttraumatic Stress-Arousal (PTS-AR), Posttraumatic Stress-Total (PTS-TOT), Sexual Concerns (SC), Anxiety (ANX), Depression (DEP), Dissociation (DIS), and Anger/Aggression (ANG).
In a multi-site sample of 219 traumatized children, the TSCYC scale was reliable and predictive of exposure to childhood sexual abuse, physical abuse, and witnessing domestic violence (1213).
The questionnaire was translated into Korean by two child and adolescent psychiatrists in our department. After a consensus procedure the questionnaire was sent to a translator for back-translation. The back-translation was then compared with the original and a final version with minor differences was sent to, and accepted by the Psychological Assessment Resources, Inc. (PAR), a copyrighter of the original scale (13).
Child behavior checklist (CBCL)
The CBCL was used for the purpose of assessing concurrent validity. The CBCL-Korean version is a widely used 132-item behavior rating scale for children ages 4-18 (16). Behaviors are rated by caretaker on a 3-point scale (0=not true, 1=somewhat true, 2=often true) over a 6-month time period. The CBCL divides behavior problems into internalizing and externalizing problems. Internalizing problems include withdrawal, somatic concerns, depression, and anxiety. Externalizing problems include aggression, delinquency, and conduct problems. It has good reliability and validity. In previous study, the CBCL Anxiety/Depression and Aggression scale were most related with TSCYC Anxiety (ANX), Depression (DEP), and Anger/Aggression (ANG) scales, respectively (17).
Child sexual behavior inventory (CSBI)
The CSBI is a measure that utilizes parent report of sexual behavior in children ages 2 to 12 yr (18). It is intended for use in the evaluation of children who have been sexually abused or who are suspected of having been sexually abused. It assesses a wide range of sexual behavior that cover a number of domains, including boundary problems, exhibitionism, gender role behavior, self-stimulation, sexual anxiety, sexual interest, sexual intrusiveness, sexual knowledge, and voyeuristic behavior. The full version of the CSBI consists of 38 items and three clinical scales (CSBI Total, Developmentally Related Sexual Behavior [DRSB], and Sexual Abuse Specific Items [SASI]) (19). Korean version of the CSBI is a reliable and valid tool which can be applied in the clinical field for assessing the sexual behavior of Korean children aged from 6 to 12 who are suspected to have been sexually abused (20). The CSBI also was used for the purpose of testing concurrent validity of the TSCYC Sexual Concerns (SC) scale (131720).
Statistical procedures
To evaluate internal reliability of the TSCYC in a Korean sample, we calculated Cronbach's alpha coefficients for the total score and for each clinical scale. A standard of 0.90 or higher was considered excellent (21). Test-retest reliability was evaluated using Pearson r. The relations between the total score and the clinical scales also were examined using Pearson r. The P value below 0.05 was considered statistically significant and Pearson r above 0.7 has been evaluated as having highly very strong positive correlation, r between 0.4-0.7 as moderate positive correlation, r between 0.2-0.39 as mild positive correlation and r below 0.2 as weak correlation (21).
The comparisons of the TSCYC total score and subscale scores between normative and traumatized group were examined using independent sample t-test. Statistical analysis was performed with SPSS/Windows (Version 15.0) (P<0.05).
RESULTS
Reliability
Internal consistency
The internal consistency for the total scale was 0.92 for the normative and 0.96 for the clinical group. The Cronbach's alpha for the clinical scales varied between 0.82 (DIS) and 0.46 (PTS-I) in the normative group, and between 0.90 (DIS) and 0.77 (PTS-I) in the traumatized group (Table 2).
Test-retest reliability
Test-retest reliability (N=88) was determined as follows for the indicated scales (ANX r=0.67, DEP r=0.65, Anger r [ANG]=0.52, PTS-I r=0.62, PTS-AV r=0.60, PTS-AR r=0.66, DIS r=0.96, and SC r=0.60). RL was r=0.95, and ATR was r=0.74 (Table 3).
Validity
Scale intercorrelations
The TSCYC clinical scale intercorrelations in the normative group ranged from 0.36 (for the DIS scale with PTS-AV scale) to 0.90 (PTS-AV with Posttraumatic-Total). As expected, the RL scale was negatively correlated with all scales, ranging from -0.36 with the ATR scale to -0.66 with the ANX scale. The correlations between all the subscales are presented in Table 4.
Concurrent validity
In the normative group, 299 caretakers also had completed the CBCL and the CSBI. All correlations were statistically significant among the TSCYC 11 subscales, the CBCL Anxious/Depressed, the CBCL Aggressive behavior and the CSBI Total (P<0.001). The TSCYC ANX (r=0.54) and DEP (r=0.49) scales were most related to the CBCL Anxiety/Depression scale. The TSCYC Anger/ANG (r=0.53) scale was most correlated with the CBCL Aggressive behavior scale. The TSCYC SC scale was most related to the CSBI Total among CBCL Anxious/Depressed (r=0.23), CBCL Aggressive behavior (r=0.23) and CSBI Total (r=0.25). However, the correlation was low and the TSCYC DEP (r=0.36) and DIS (r=0.36) were most related to the CSBI Total. The Pearson's correlations are shown in Table 5.
Differences between the normative group and the sexually traumatized group
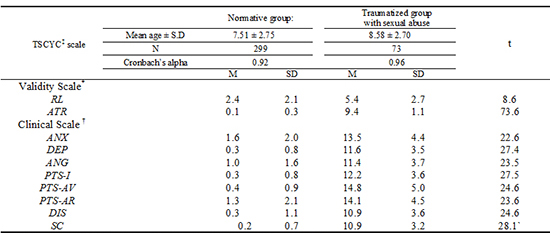
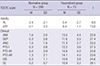
As shown in Table 6, there were significant differences between the normative and the traumatized group on all of the clinical subscales. In normative group, the 8 clinical scale and 2 validity scales did not differ significantly by either age or sex.
DISCUSSION
This study shows that the TSCYC can be translated and used outside English speaking societies, while still keeping its psychometric properties. This is the first study using the TSCYC in Korean population.
The psychometric properties of the Korean translation of the TSCYC seem to be good. In our study, concerning internal consistency, coefficient alpha for mean clinical scales were 0.92 and 0.96 each for the normative group and the traumatized group with child sexual abuse. Original author, Briere reported coefficient alpha for mean clinical scales was 0.86 for the standardization sample (N=750) and 0.87 for the validation sample (N=213) (13). Nilsson et al reported coefficient alpha of the Swedish version of the TSCYC for mean clinical scales were 0.93 and 0.96 each for the normative group and the traumatized group (22). In Swedish sample, 59 children in traumatized group had experienced sexual abuse and/or physical abuse, while some had also witnessed violence in their home (22). The internal consistency of the Korean version of the TSCYC was higher than results by the original author and similar to the Swedish version (). Moreover, the internal consistency in our traumatized group was higher than normative group in all clinical scales and in Response Level validity scale. For clinical scales, the coefficients alpha of in normative group was ranged from 0.57 to 0.90 in our study and from 0.55 to 0.88 in the Swedish sample (22). In the traumatized group, it was ranged from 0.77 to 0.96 in our study and 0.77 to 0.93 in the Swedish sample, which was very similar to our results (22). In validation sample in Briere's study, the coefficients alpha was ranged from 0.86 to 0.93 (13).
Among validity scales, coefficient alpha for the ATR scales was low, 0.57 for the normative group and 0.35 for the traumatized group. In Briere study, coefficient alpha for the ATR scale also was low, 0.36 for the traumatized sample (N=213) and 0.46 for the Gilbert sample (N=433) (1317). In the Swedish sample, it was 0.36 for the normative group (N=629) and 0.12, very low for the traumatized group (N=59) (22). In our study, coefficient alpha for the ATR scales was similar to the original validation study and much better than the Swedish sample. Atypical responding rarely reflects an underlying latent construct, but rather shows a tendency to respond to items that otherwise have a low base-rate of acknowledgment. As results, coefficient alpha of infrequently acknowledged items are typically low due to a limitation in score range (13). In general, the internal consistency of the Korean version of the TSCYC was satisfactory in both the normative and traumatized group.
In our study of the test-retest reliability, correlations were ranged from 0.52 to 0.96 (N=88), while they were from 0.68 to 0.96 in Briere's study (N=33) (13). In the Swedish sample, correlations were ranged from 0.56 to 0.95 (N=26) (22). In Swedish study, retest had been done after 2 weeks and in our study it had been done in 4 weeks. Although the coefficient for the ATR scales was noncalculable because all respondents scored "9" on the second occasion in Swedish test-retest sample, it was r=0.74 in our study. The coefficient for the RL validity scale was r=0.79 in Swedish sample, and better, r=0.95 in our study. The test-retest reliability of Korean version of the TSCYC was found to be compatible with the original scale and the Swedish version. Two validity scales, the Response Level scale and the Atypical Response scale, are unique strength of the TSCYC and coefficient alpha and test-retest correlation in two validity scales were better in our study, which meant that Korean version of the TSCYC were reliable.
When compared with the comparable scale of the CBCL, concurrent validity of the depression (r=0.49) and anxiety scale (r=0.53) was moderately correlated. Although SC scale was also significantly correlated with the scores of the CSBI, association was very mild (r=0.25). In previous study, association was ranging from 0.55 to 0.82 with three parent/caretaker-report measures such as the CBCL, the CSBI and the Child Dissociative Checklist (1317).
There were significant differences between the normative group and the traumatized group on the total scale and all the clinical scales. In Briere's study, means and standard deviations in 8 clinical scales were between 9.8±2.4 for sexual concern and 13.6±4.2 for PTS-AR in traumatized group (N=317). In our study, they were similar between 10.9±3.2 for SC and 14.8±5.0 for PTS-AV in traumatized group (N=73). However, means and standard deviations in 8 clinical scales were much lower between 0.2±0.7 and 1.6±2.0 in normative group (N=299) in our study than between 9.3±1.1 and 11.8±3.3 in normative group (N=433) in Briere's study. Because of stigma for mentally ill patients, Korea was the one of the countries showing response bias toward giving the most socially desirable answer and lower means at clinical measures (1123). In spite of socially desirable manner among Korean, similar means in traumatized group in both study support good discriminant validity of the Korean version of the TSCYC. These findings gave support for this scale of the TSCYC as valid.
Symptoms of posttraumatic stress disorder (PTSD) are common sequelae of child sexual abuse. There are several obstacles to the assessment of long term mental health effects of child sexual abuse. Child victims may deny that the abuse event occurred, may be too ashamed about the event to report its impact, and may have difficulty with direct questioning. Therefore, the parents' reports of symptoms are critical in the assessment of PTSD. Many children in our traumatized group had PTSD symptoms and higher PTSD scale scores compared with normative group. For these reasons, the TSCYC may be used as an economical and time-efficient screening device for PTSD in traumatized children, especially sexually abused group (242526).
Although Briere has made divisions with ages 3-4, 5-9 and 10-12 and revealed main effects of child gender, there had been no significantly difference between sex and ages in normative group in our study (12). Small sample size in younger age and relatively very low means in normative group could be the cause of no difference between sex and age.
Our study has some limitations. The study sample is not a representative national sample since the other cities in Korea did not take part in the study. One major limitation of this study is that no other measure of PTSD was administered. Also, the traumatized group in our study was mostly sexually abused children coming from one Sunflower Center for evaluation and treatment. When viewed from perspective from the TSCYC original intent, the traumatized group also included accident and witnessed domestic violence. In the future direction, we need Korean national norms, raw score to T-Score and percentile conversion according to age and sex with large representative national sample. Considering that post-traumatic stress, dissociation, and sexual concerns support the construct validity of the TSCYC, it is recommended to correlate the TSCYC with other PTSD scale, dissociative scale for children and specific sexual concern items in the CSBI (2132728293031). The lack of information on the traumatic events using other traumatic events scales in normative group was also considered to be a limitation.
For the child younger than 8 yr old or for the child with limited cognitive development, the TSCYC should be used and dependent on the caretaker's report. However, the parents who suffer from post-traumatic symptoms or depressive symptoms have limited ability to report their own children's symptom. The usage of the TSCYC has better accompany the evaluation of parents.
Nevertheless, our study is meaningful (considered discriminant validity) in its potential use with children too young to report on their own internal state of symptomatology and diagnostic tool for screening PTSD with child sexual abuse. The Korean TSCYC can be applied for younger children with insufficient cognitive development, or lack the reading comprehension necessary to respond to written test items.


 XML Download
XML Download