

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neuropathic pain is defined as "a pain caused by a lesion or disease of the somatosensory system" according to the International Association for the Study of Pain (1). Neuropathic pain is diagnosed by an expert physician based on a detailed clinical history, physical exploration, and clinical judgment as well as by electrophysiological examinations and imaging studies as needed (2).
However, it is difficult to distinguish neuropathic pain from other types of pain and to diagnose the lesion or disease causing the pain (2). Moreover, an accurate diagnosis of neuropathic pain requires training and experience, which is time-consuming. Early identification of neuropathic pain in primary and specialty care settings would avoid unnecessary delays in the improvement of symptoms (3). Therefore, easy-to-screen questionnaires for neuropathic pain in patients with chronic pain would be of great clinical benefit.
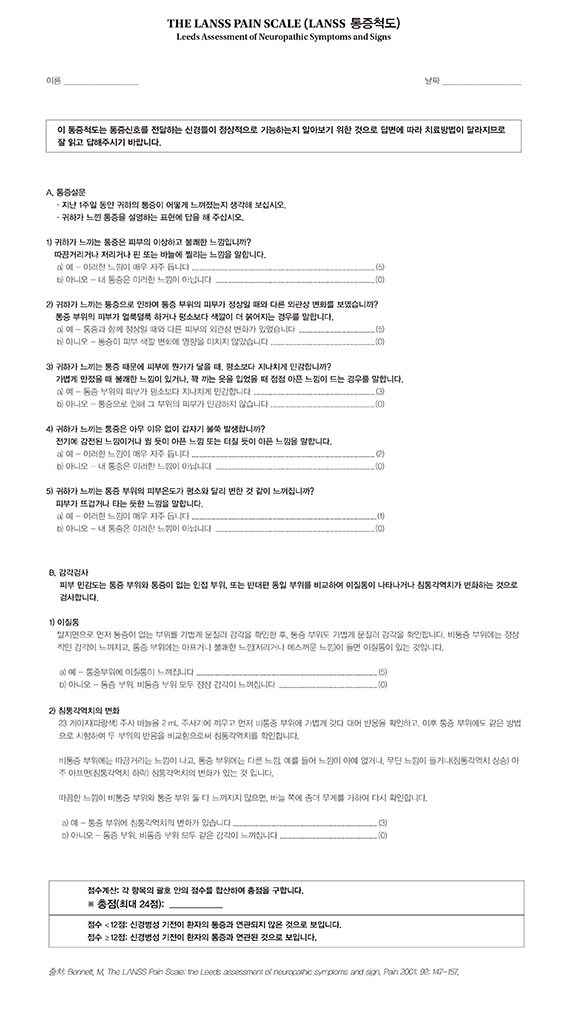
The Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) pain scale, a screening questionnaire for identifying patients with neuropathic pain, was developed to identify patients with neuropathic mechanisms dominating their pain experience (4). The LANSS pain scale is comprised of 7 items divided into 5 symptoms and 2 signs. It is concordant of clinical diagnosis with a sensitivity and specificity of 83% and 87%, respectively, and a score of at least 12 of 24 points (4). The original English version of the LANSS pain scale has been translated and validated in Turkish (5), Spanish (6), Swedish (7), Brazilian Portuguese (8), Portuguese (9), and Chinese Mandarin (10). However, no neuropathic pain questionnaire including the LANSS has yet been established in Korea.
Although these screening tools are based on descriptors, their linguistic adaptation and validation into different languages are feasible and this ensures their reliability and validity in languages other than those in which they were initially developed (11). As cross-border and cross-cultural studies continue to increase, there is a greater need for linguistic validation across a variety of societies. In order to use questionnaires in areas with different languages and cultures, not only translation into new languages is required, there is also a need for adaption of questionnaires to suit regional characteristics. The aim of this study was to translate and adapt the LANSS pain scale into Korean and to investigate the reliability and validity of the Korean version of the LANSS (K-LANSS) pain scale.
MATERIALS AND METHODS
This study had 2 stages. First, the English version of the LANSS was translated into Korean, and the K-LANSS was developed through cross-cultural adaptation. In the second stage, the reliability and validity of the K-LANSS were examined in patients visiting the outpatient department for pain management.
Development of the K-LANSS
The translation and cross-cultural adaptation process of the LANSS pain scale was carried out based on the guidelines put forth by Beaton et al. and Guillemin et al. (Fig. 1) (1213). Two native Korean translators fluent in both English and Korean each completed a separate forward translation from English to Korean. One forward translator was an informed pain physician and the other was an uninformed non-physician. The two versions were synthesized into a single Korean version by the two translators. This synthesized version of the Korean LANSS was then given to two independent native English-speaking translators also fluent in Korean, for back translation into English. One back translator was an uninformed pain physician and the other was an uninformed non-physician. An expert committee composed of forward translators, back translators, and 5 pain specialists reviewed the forward translation, the synthesized version of the Korean LANSS, the back translation, and the original version of the LANSS. This expert committee produced the pre-final version of the K-LANSS focusing on linguistic and cultural differences. Discrepancies were resolved by consensus to achieve conceptual equivalence with the original questionnaire. The pre-final version of the K-LANSS was field-tested on 20 patients. After completion of the questionnaire, each question was discussed with the patient to determine whether all items had been fully understood and to understand whether the patients had any problems with the formulation. The final version of the K-LANSS was created reflecting the problems identified and was verified by the committee (Appendix 1).
The K-LANSS pain scale is based on an analysis of the sensory description and bedside examination of dysfunction. It is comprised of 5 symptoms and 2 clinical examinations. The first part consists of 5 dichotomous questions asking the patient what kind of pain he or she experienced in the last week. The second part consists of a sensitivity examination, through which the health professional explores skin sensitivity, comparing the painful area with a non-painful contralateral or adjacent area. The presence of allodynia and altered pinprick perception threshold are explored. The possible scores range from 0 to 24.
Clinical study for reliability and validity of the K-LANSS
In order to measure reliability and validity of the K-LANSS, an observational study was designed to be carried out under the normal conditions of clinical practice. Patients who visited the outpatient department in 1 of 2 tertiary university hospitals for pain management between June 2014 and December 2014 were screened by the following criteria. The inclusion criteria were as follows: age of 20 yr or older; 11-point numeric rating scale (NRS) pain score ≥4; and able to speak and write Korean. The exclusion criteria were as follows: uncertain diagnosis; mixed pain presentation, visceral pain, or fibromyalgia; depression, alcoholism, or drug abuse; inability to understand or read the questionnaire; and visual impairment.
Differential diagnosis of patients regarding neuropathic or nociceptive pain was initially made by 2 independent pain specialists in each separate hospital. The diagnosis was based on medical history, detailed clinical examination, neuroimaging, electrophysiological studies and laboratory tests (14). Neuropathic pain was determined by clinical and laboratorial tests, which included identification of abnormal sensory perception, such as postherpetic neuralgia or peripheral neuropathy. Nociceptive pain was diagnosed by the clinical and/or laboratorial evidence of nonneuronal tissue damage, such as myofascial pain syndrome, and/or with normal electrophysiological studies. The patient was included in the clinical study only if 2 independent pain specialists concurred in the diagnosis of pain type. Subsequently, another researcher blinded to the pain classification of the participants, had the subjects answer the K-LANSS and collected data about the patients pain such as their NRS pain score and duration of pain and also about their socio-demographic characteristics such as age, gender, occupation, education level, and routine medical information.
Statistical analysis
Generally, a sample size of at least 50 patients is recommended for a reliability test. For an exploratory factor analysis, 7 patients per item and at least 100 patients are recommended (15). Thus, a sample size of at least 100 patients in each group was required. Descriptive statistics were used to describe demographic characteristics. The normality of the data distribution was assessed using the Kolmogorov-Smirnov test. Comparisons were made with the independent t-test, Mann-Whitney U test, chi-square test, and Fisher's exact test as appropriate. Reliability was assessed by analysis of internal consistency and exploratory factor analysis. Internal consistency measures the consistency of each item on the same questionnaire. The relationships between different items were estimated by measuring Cronbach's α coefficient. Split-half reliability, a subtype of internal consistency reliability, was assessed by computing the Guttman split-half coefficient. Validity was assessed by the receiver operating characteristic (ROC) curve, sensitivity, specificity, positive predictive value, and negative predictive value. SPSS 18.0 (SPSS Inc., Chicago, IL, USA) and MedCalc 12.5.0.0 (MedCalc Software, Mariakerke, Belgium) were used for the statistical analysis. A 2-sided P value < 0.05 was considered statistically significant.
Ethics statement
The patients were informed regarding this study, and written informed consent was obtained from all participants prior to enrollment. The study protocol was approved by the institutional review board of Severance Hospital (ref: 4-2014-0280) and Gangnam Severance Hospital (ref: 3-2014-0086).
RESULTS
Development of the K-LANSS
Though there were no serious linguistic problems during the LANSS pain scale translation, the authors found some minor discrepancies, which could be resolved by cross-cultural adaptation. First, shades of meaning exist between Korean and English when people answer the question by 'Yes' or 'No.' In the Korean language people answer 'Yes' or 'No' in the place of the questioner. Therefore, the 'Yes'-'No' order of answer is more familiar to the Korean user. The 'No'-'Yes' order of answer in the original LANSS pain scale was modified to a 'Yes'-'No' order. In addition, most native Koreans consider skin tone to be of a yellow hue, and do not use the expression 'pink skin'. Therefore, the second item in the first section of the LANSS, "looking more red or pink" was revised to "looking more red."
Clinical study for reliability and validity of the K-LANSS
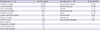
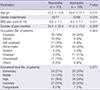
A total of 213 patients eligible for inclusion in the study were evaluated, of which 113 were diagnosed with neuropathic pain, and 100 with nociceptive pain (Table 1). There were no significant differences of socio-demographic and clinical characteristics between the neuropathic pain and nociceptive pain groups except duration of pain, which was shorter in the neuropathic pain group (Table 2).
The mean overall score of the K-LANSS pain scale attained from the neuropathic and nociceptive pain groups was 15.3±6.5 and 3.3±3.8, respectively, with significantly higher scores in the neuropathic pain group (P<0.001). Cronbach's α coefficient for assessing internal consistency of the whole K-LANSS was 0.815 (Table 3), and the Guttman split-half coefficient was 0.800.
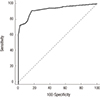
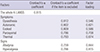
The ROC curve of the K-LANSS pain scale is shown in Fig. 2. The area under the ROC curve (AUC) was 0.928 with a 95% confidence interval (CI) of 0.885-0.959 (P<0.001). When the cut-off value of the original version, ≥12, was applied, the sensitivity was 72.6% (95% CI, 63.4-80.5), specificity was 98.0% (95% CI, 93.0-99.8), and the positive (PPV) and negative predictive values (NPV) were 98% and 76%, respectively (Table 4). The best cut-off point obtained by ROC curve analysis was 7, and the Youden index was 0.742. Corresponding to this point, sensitivity was 91.2% (95% CI, 84.3-95.7), specificity was 83.0% (95% CI, 74.2-89.8), and PPV and NPV were 86% and 89% respectively (Table 4). The kappa value was 0.694 (P<0.001) which was computed for valuation of the concordance between clinical diagnosis and the diagnosis from the K-LANSS pain scale.
DISCUSSION
This study demonstrated that the K-LANSS pain scale has good reliability and validity as a neuropathic pain assessment tool. To the best of our knowledge, this is the first attempt to translate and study the validity of a neuropathic pain screening questionnaire in Korea. Although the Korean Neuropathic Pain Questionnaire for neuropathic pain screening and grading has already been developed in Korea (16), its specificity was somewhat low according to a pilot study, and it has not yet gained much domestic acceptance.
Neuropathic pain is known to impair quality of life and is more costly to treat than other pain conditions (17). Therefore, the identification of neuropathic pain is a critical first step in designing appropriate therapeutic strategies and improving the quality of life for patients. However, complicated and variable clinical manifestations of neuropathic pain make the diagnosis quite challenging, as the symptoms often appear differently at each stage of the disease, and lesions of the somatosensory nervous system are difficult to detect (218). Against this backdrop, many questionnaires for neuropathic pain screening have been introduced, and the LANSS pain scale developed by Bennett is a very useful test that provides immediate clinical information and helps differentiate nociceptive pain from neuropathic pain (4).
In this study, internal consistency analysis was used to assess the reliability of the K-LANSS. The Cronbach's α value of the K-LANSS was 0.815, indicating satisfactory internal consistency. This value exceeds the values for the Spanish (0.68) (6), Brazilian Portuguese (0.67) (8), and Portuguese versions (0.78) (9) and is consistent with the values for the Turkish (0.841) (5) and Chinese Mandarin versions (0.824) (10). After additional analysis using the split-half method, the Guttman split-half coefficient value was 0.800, greater than the suggested cut-off of 0.7 and equivalent to the value of the Chinese Mandarin version (0.842) (10). Performing appropriate interventional mangement or beginning administration of medicine is general clinical practice in the hospitals to which the authors belong, depending on the diagnosis of the patients visiting the outpatient clinic. Therefore, the test-retest findings used to assess the consistency of a measure from one time to another could have been affected by individual patient treatments. Thus, test-retest analysis was not carried out.
Regarding validity, the AUC provides a critical estimate of the expected accuracy of a test (19). In our study, the AUC of the K-LANSS was 0.928, using expert clinical diagnosis as the gold standard. In the original version of the LANSS pain scale, the sensitivity and specificity were 83% and 87% respectively, and the best cut-off value for discrimination of neuropathic pain was 12. The sensitivity and specificity in the K-LANSS using the original cut-off value of 12 were 72.6% and 98.0%, respectively, representing slightly lower sensitivity and slightly higher specificity than the original version. When using a cut-off value of 7, which is the optimal cut-off value obtained by making a graph of the ROC curve in the K-LANSS, the sensitivity and specificity were 91.2% and 83.0%, respectively. The kappa value, an indicator of the diagnostic concordance rate, was 0.694, higher than the 0.65 value of the original version. In conclusion, these results suggest that the K-LANSS displays high validity.
In the present study, patients with mixed pain were excluded. In cases with symptoms such radiculopathy and nerve entrapment with pain presentation caused by neuropathic and/or nociceptive mechanisms, a definite diagnosis of pain with only a neuropathic component was required for inclusion in the neuropathic pain group. We excluded patients with mixed pain presentation, because there was no way to distinguish pain types, and no mixed pain group was used in the original study.
There was some concern that the use of a cutting needle such as 23-gauge needle may cause bleeding when the LANSS pain scale was applied to patients (20). However, no patients with injury by the 23-gauge needle examination were found, and we believe the pinprick test of this scale is safe.
The present instrument is simple, easy, and less time-consuming for both patients and physicians. Therefore, it may be useful for patients with neuropathic pain who have poor patient compliance on questionnaires, and it can be a readily employable screening tool for physicians who find it difficult to conduct a comprehensive assessment.
This study has some limitations. First, although patients with neuropathic and/or nociceptive pain also visit departments of neurology, orthopedics, and neurosurgery for diagnosis and treatment of disease, we recruited patients who visited the outpatient department for pain management. However, the authors believe that the findings of the present study are generalizable, because 2 tertiary university hospitals were involved in the research. Nevertheless, this study could have more representation power if it was a multicenter study including a primary care clinic. In addition, further research is needed for more definitive results in order to make conclusions regarding epidemiologic information. Second, because there are no other Korean versions of questionnaires for screening of neuropathic pain except for the K-LANSS, we could not test convergent validity. We expect that the findings of this study will help with the development of Korean versions of other neuropathic pain questionnaires. Third, the committee in this study consisted of forward translators, back translators, 5 pain specialists, but no linguistic specialists. Although supervision of a linguist would have made the K-LANSS more reliable and valid, the authors deliberated on linguistic features and cultural background for development of the K-LANSS. Before all, because in each item of the original LANSS the example follows main question, it suggests simple and typical expression describing applicable pain. Therefore, the authors suppose this limitation not so crucial to the findings of this study in spite of the exclusion of linguistic specialists in the committee during translation and adaptation.
In conclusion, this study confirmed that the K-LANSS is a useful, reliable, and valid questionnaire for discrimination of neuropathic pain from nociceptive pain. The K-LANSS is the first Korean version of a screening questionnaire for patients with neuropathic pain. We hope that the K-LANSS will not only come into widespread use as a screening tool, but also provide objective information for the study of neuropathic pain with support from the results of this study.

 XML Download
XML Download