

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For patients with high-risk renal cell carcinoma (RCC), proposed benefits of lymph node dissection (LND) at the time of nephrectomy include more precise assessment of prognosis by accurate staging, decreased local and/or systemic recurrence, and longer survival (1). Although most patients with pathological lymph node involvement (LNI) also have distant metastatic disease, in approximately 3% to 10% of RCC patients in modern series, spread is confined to LNs (23). Patients with only nodal metastases (pTanyN1M0) are a distinct cohort for which surgical treatment of the primary tumor plus LND may result in durable disease-free survival (24). Furthermore, stage shifting in RCC may result in more patients who have only early LNI and could benefit from removal of these lesions (5). Accurate staging is also important for identifying patients who are at high risk of recurrence and for enrollment in ongoing clinical trials of adjuvant targeted therapies. However, there is no consensus on the effectiveness of LND or a dissection template for RCC because of its relatively heterogeneous metastatic spread (6).
Several studies have investigated selection of RCC patients at heightened risk for regional LNI based on clinical and/or pathological factors (7). The most informative preoperative predictors for LNI are clinical tumor size, advanced clinical T stage, radiological positive nodes, metastasis at diagnosis and symptom classification (89). Clinical lymphadenopathy at preoperative imaging (cN1) has been reported to harbor pathologic LNI in 42% of cases, indicating its use as a high risk factor (10). However, available imaging techniques do not reliably predict nodal metastases (1112). An upper limit cutoff value of 1 cm for normal nodes results in 10% false negatives due to micrometastases (111213) and false-positive rates of 3% to 58% mainly because of reactive inflammatory nodal enlargement that is found most frequently in patients with renal vein invasion and tumor necrosis (10).
This study evaluated the diagnostic and prognostic value of clinical positive nodes on computed tomography (CT) in patients with RCC without distant metastases who underwent nephrectomy and LND. Agreement between clinical and pathological N stage was evaluated and oncological outcome of the cohort were compared after stratification by clinical and pathological nodal status. We also identified which patients undergoing LND were at high risk of harboring LNI, information needed to correctly stage and adequately plan treatment.
MATERIALS AND METHODS
Records for 440 patients with cTanyNanyM0 RCC of any histological subtype who were treated with nephrectomy with LND between 1994 and 2013 at our institution were retrospectively analyzed. Patients with fewer than 12 months of follow-up, a history of previous RCC or synchronous bilateral tumors, or Von-Hippel Lindau disease were excluded. Of the 440 patients with RCC without distant metastases at initial presentation and who underwent LND, 102 (23.2%) had cN1 disease and 338 (76.8%) had cN0 disease. Baseline characteristics of the study cohort stratified by clinical node status are listed in Table 1.
The American Society of Anesthesiologists (ASA) scores were assigned by anesthesiologists. Before nephrectomy, all patients were staged preoperatively with cross-sectional abdominal CT imaging and chest imaging by X-ray or CT. Radiographic information such as tumor and LN size, presence of tumor necrosis or tumor thrombus, and tumor location was collected. Clinical tumor size was defined as the greatest tumor diameter in cm on cross-sectional imaging. We defined cN1 as presence of at least one radiologically detected lymphadenopathy (>1 cm) in the retroperitoneal lymphatic area on preoperative CT imaging. Bone and brain scan assessments were performed in patients at high risk for bone or brain metastases.
LND was performed at the time of nephrectomy, and the dissection template was not standardized during the study period among the multiple surgeons. The decision to perform LND and LND extent were decided by the urologist performing the surgery according to clinical characteristics and surgeon preference. Operative reports were reviewed for each patient to confirm LND and presence of enlarged LNs at the time of surgery. The LN template was categorized as only ipsilateral hilar regional (n=246, 55.9%) or as other, including paracaval, precaval, retrocaval and interaortocaval for right-sided tumors and paraaortic, preaortic and interaortocaval for left-sided tumors (n=194, 44.1%). Patients with incidental perinephric nodal tissue discovered only in the nephrectomy specimen were considered to be LND-negative.
Tumor stage was reassessed according to the seventh edition of the American Joint Committee on Cancer (AJCC) TNM classification (14). All tumors were graded using the Fuhrman nuclear grading system. Histological tumor necrosis was defined as any microscopic coagulative tumor necrosis. Sarcomatoid component was defined as a spindle cell malignancy with the histological appearance of a sarcoma. Capillary-lymphatic invasion (CLI) was used to define tumors in microscopic capillary or lymphatic channels in lacking a muscular coat (15). All removed LNs were examined for the presence of nodal metastases. Specific nodal parameters included total number of nodes removed and number of positive nodes.
CT or abdomen ultrasonography plus chest X-ray was performed on patients according to risk profile at each visit. Distant metastasis was any recurrence outside of the retroperitoneum. Metastasis-free survival (MFS) was calculated in months from the date of surgery to the date of distant metastasis. To analyze cancer-specific survival (CSS), data on causes and dates of death were obtained from the Korea National Statistical Office and internal chart review. CSS was calculated in months from the date of surgery to the date of final follow-up or death due to RCC progression.
Patient and tumor characteristics were compared between patients with clinically node negative or positive RCC using chi-square test for categorical variables and Student's t-test for continuous variables. Outcome measures including MFS and CSS were estimated using the Kaplan-Meier (KM) Method, and the log-rank test was used to compare survival differences according to stratified clinical and pathological nodal status. Multivariate Cox proportional hazards regression analysis was performed to determine significant predictors of MFS and CSS using variables that were statistically significant in univariate analysis. Finally, univariate analysis was performed to determine significant covariates between pN1 and pN0 patients; these covariates were then used in a multivariate logistic regression model to determine predictors of pathology LNI. P-values were two-sided and P<0.05 indicated statistical significance. Analyses used SPSS, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Of the 440 patients, 246 (55.9%) underwent hilar LND while 194 (44.1%) underwent other LND. The mean number of LNs examined was 8.3 (range 1-62), with node-positive disease identified in 31 (7.0%) patients. The mean number of nodes sampled was 8.1 for the node-negative group, with a maximum of 52 sampled, and 8.9 for the node-positive group, with a maximum of 62 sampled (P=0.43). Patients with cN1 disease had more unfavorable clinical and pathological characteristics than patients with cN0 disease (Table 1). Patients with clinically positive nodes were more likely to have larger tumor size (P<0.001), tumor thrombus (P=0.008), higher proportion of papillary histology (P=0.009), higher T stage (P<0.001), higher nuclear grade (P<0.001), a sarcomatoid component (P<0.001) and CNI (P<0.001). LNI prevalence was 19.6% in patients with suspicious nodal metastases at preoperative imaging while 3.3% of patients with cN0 disease had pathologically LN-positive disease (P<0.001). We calculated 65% sensitivity, 80% specificity, and 77% accuracy for LN staging by preoperative CT.
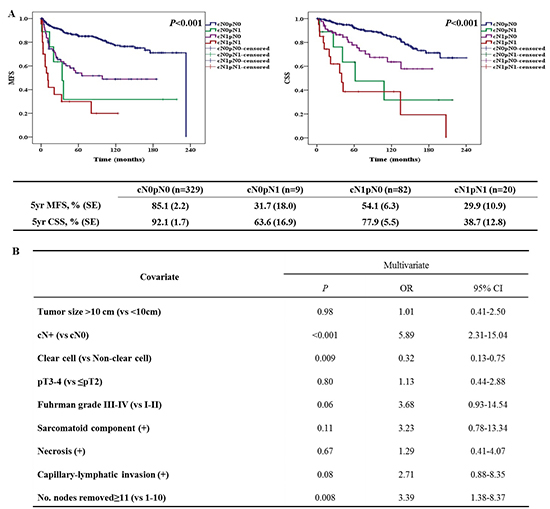
During a median follow-up of 69 months, distant metastasis occurred in 111 patients (25%), with 83 cancer-specific deaths (18.9%). Five-year MFS was 83.6% and CSS was 91.3% in patients with clinically negative LNs; MFS was 49.2% and CSS was 70.1% in patients with clinically positive LNs, with worse prognosis among patients with clinically positive nodes (all P<0.001, Fig. 1A, B). MFS and CSS were also significantly different for pN0 and pN1 patients (Fig. 1C, D, P<0.001). When survival outcomes were further stratified by clinical and pathological nodal status, 5-yr MFS (Fig. 2A) and CSS (Fig. 2B) were 85.1% and 92.1% in cN0pN0 (n=329, 74.8%) patients, respectively; 54.1% and 77.9% for cN1pN0 patients (n=82, 18.6%); 31.7% and 63.6% for cN0pN1 (n=9, 2.0%) patients; and 29.9% and 38.7% for cN1pN1 (n=20, 4.6%) patients (all P<0.001). Differences in MFS and CSS between the cN0pN0 and cN1pN0 groups were significant (all P<0.001) while survival outcomes of cN1pN0 and cN0pN1 patients were comparable (P=0.47 for MFS and P=0.12 for CSS) (Fig. 2).
After adjustment for all other covariates, cN1 was identified as a significant predictor of MFS (P<0.001; hazard ratio [HR], 2.47) and CSS (P=0.009; HR, 2.04) (Table 2). In subgroup analysis of pN0, clinical lymphadenopathy was associated with poor prognosis (MFS, HR 2.27, P<0.001; CSS, HR 2.05, P=0.02). When the prognostic significance of cN stage was examined in stage-for-stage and grade-for-grade analyses (Table 3), patients with cN1 cancer showed significantly lower MFS and CSS rates than patients with cN0 cancer in the advanced disease category (pT3 or pT4) (P=0.001, HR 2.66 for MFS and P=0.02, HR 2.45 for CSS) after adjustment for all other covariates. When the prognostic significance of cN stage was determined by grade in subgroup analysis, cN1 was a significant predictor of MFS and CSS for all grades relative to their pN0 counterparts (all P<0.05). Finally, the most informative independent predictors of pathological LN metastasis were clinical nodal status (cN1 vs cN0, odds ratio [OR] 5.89, P<0.001) (Table 4).
DISCUSSION
LND rates for RCC have declined in the past decade because of the rapid growth of minimally invasive techniques and a lower incidence of radiographic lymphadenopathies (16). However patients with isolated regional nodal metastases from RCC are a distinct cohort for whom resection of involved LNs might provide therapeutic benefits (24). Furthermore, the detrimental effects of nodal metastases on cancer-specific mortality after nephrectomy are particularly high in patients with low-stage or low-grade non-metastatic RCC (17). We similarly found that in grade-for-grade analyses, Fuhrman Grade (FG) I-II and FG III-IV patients with cN1 disease were 4.1-fold, 2.5-fold, 6.5-fold, and 1.9-fold more likely to have metastatic recurrence or cancer-specific death relative to cN0 counterparts.
The aim of our study was to investigate the diagnostic and prognostic value of positive LNs on preoperative CT imaging and to identify specific subsets which might benefit from aggressive surgical resection involving LND. Predictive nomograms for LNI have been developed to prevent unnecessary LNDs and ensure adequate extension of LND templates to high-risk cases, incorporating symptoms, radiographic lymphadenopathy, intraoperative palpable LNs, tumor stage of ≥pT3, presence of sarcomatoid features, nuclear grade ≥3 and histological necrosis (18192021). Non-clear cell subtype and removed LNs ≥11, cN stage based on CT imaging was the most informative predictor of LNI in our cohort, which confirmed the findings of previous study (21).
LNI rates vary considerably regarding the presence of distant metastases and the extent of LND (79). In our results, the overall pN1 rate (7.0%) was comparable to rates reported in previous studies (2.9%-6.1%) based on data from patients with M0 RCC treated with LND (8922). We found that most patients with nodal metastases (65%) had clinically node-positive disease identified on preoperative imaging. Furthermore, the presence of clinical lymphadenopathy had a detrimental effect on MFS and CSS that was strongly stratified with pathological characteristics of pT stage, pN stage and nuclear grade. Patients with clinically positive but pathologically negative LNs (cN1pN0, 18.6%) had similar survival outcomes to patients with clinically negative but pathologically positive LNs (cN0pN1, 2.0%). However, these patients had a worse prognosis than patients with clinically and pathologically negative LNs (cN0pN0, 74.8%), consistent with a previous report (21), implying the prophylactic effects of LND via removing the means by which cancer might spread through lymphatic channels. Moreover, an inflammatory response to a tumor could be a sign of systemic dissemination or of micro-metastases in non-sampled LNs and inadequate LND. However, comparing MFS and CSS between cN0pN1 and cN1pN1 groups indicated that the absence of evident LN metastasis does not preclude regional LND because of undetected LN micro-metastasis on available imaging technology.
In the present study, LN staging by CT had a sensitivity of 65%, a specificity of 80%, and an accuracy of 77%. Prior series found only a modest association between LN size and metastatic involvement, with 32%-43% of LNs >1 cm containing metastatic disease (101823). Nodal enlargement can be caused by reactive hyperplasia, which is often associated with large or extensive tumor necrosis or venous thrombosis, and may represent a reactive immune response (10). Furthermore, micrometastases in normal-sized nodes cannot be visualized using the above mentioned techniques (111213). The evolution of CT technology such as multidetector CT with higher spatial resolution have improved diagnosis by reducing false-positives from reactive hyperplasia (12).
Here in, we did not use a standard template, and the extent of dissection might have been influenced by the risk of nodal metastases. In addition, most patients underwent only hilar LND, which could underestimate the true rate of LNI. Clearly, hilar node dissection alone, incorporating fatty tissue along the renal vessels to the vena cava or aorta, is insufficient. LN metastases without involvement of the renal hilum are common, with involvement of the interaortocaval nodes without regional hilar involvement in 35%-45% of patients (7). Improved CSS and increased number of LNs excised in nonmetastatic, LN-positive patients are significantly associated (24), and 15 LNs need to be removed to achieve a 90% probability of detecting at least one metastatic LN (25). These findings suggest that more extensive LND including retrocaval and/or interaortocaval dissection should be pursued in all patients with clinically node-positive RCC undergoing nephrectomy, regardless of technique (26).
In our study, selection bias was possible since the cohort was restricted to a single institution and contained mostly patients considered to be high-risk for LN metastasis who underwent LND. Surgeon preference and retrospective data collection from patient medical records might have affected the accuracy of variables related to the LND extent. Preoperative CT techniques were not standardized and radiology re-review was not performed, which could have affected the accuracy of cN staging. Finally, using the operative records, we were unable to assess factors affecting surgeons' intent to perform retroperitoneal LND (RPLND) for cN0 disease such as intraoperative palpable or suspicious LNs. Additional prospective multi-institutional assessments will help evaluate our findings and further define LND as a treatment for patients with low-volume LN metastases without distant metastases.




 XML Download
XML Download