

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary computed tomography angiography (CCTA) is an emerging technique that allows high diagnostic accuracy for the detection of coronary artery disease (CAD) and high negative predictive value for the exclusion of CAD (123). In addition, negative result in CCTA provides reassuring prognostic information. No obstructive lesion in CCTA has been shown to be associated with very low adverse event rates (456). Recent study with a large cohort of 23,854 patients demonstrated that annualized mortality was 0.22% in subjects without evident CAD by CCTA (4). However, there have been limited studies focusing on clinical outcomes of subjects without obstructive CAD by CCTA. Accordingly, prognostic factors determining future events in this population remain unclear. This study was conducted to assess the clinical outcomes and parameters determining the cardiovascular events in subjects without obstructive CAD on CCTA.
MATERIALS AND METHODS
Study subjects
Retrospective analysis was performed with data from three different CCTA registries that have been launched to assess clinical utility of CCTA involving three cardiac centers in Korea (Seoul National University Hospital, Seoul; Seoul National University Bundang Hospital, Seongnam; and Boramae Medical Center, Seoul). Between November 2004 and November 2010, all study patients underwent CCTA because they were suspected of having CAD. Patients who had at least one of following criteria were excluded: 1) previous myocardial infarction (MI) and/or coronary revascularization, 2) inadequate image quality, and 3) insufficient clinical information for the study analysis. After exclusion, a total of 1,857 patients remained. Among them, 454 (24.4%), 171 (9.2%), and 1,232 (66.3%) had no (0% stenosis), non-obstructive (1%-49% stenosis) and obstructive (≥ 50% stenosis) CAD, respectively. In this study, a total of 625 with no or nonobstructive CAD by CCTA was analyzed. Information on baseline clinical characteristics, including cardiovascular risk factors and type of symptoms, was obtained by reviewing patients' medical records. Hypertension was defined as documented history of high blood pressure or use of anti-hypertensive medications. Diabetes mellitus was defined by diagnosis of Diabetes mellitus made previously by a physician or use oral hypoglycemic agents or insulin. Dyslipidemia was defined as known but untreated dyslipidemia or current treatment with lipid lowering agents (4). The pretest probability of CAD was determined by age, sex and the nature of chest pain during initial presentation (7). The pretest probabilities were classified as low (<10%), intermediate (10%-90%) and high (>90%). Chest pain was classified as typical, atypical and non-cardiac. Typical chest pain was defined as chest pain that was 1) substernal, 2) provoked by exertion or emotional stress, and 3) relieved by rest and/or nitroglycerin. Chest pain was classified as atypical if two of these features were present, and non-cardiac if one or none of these features were present (8). Renal function was estimated by estimated creatinine clearance (eCCr), which was calculated using the Cockcroft-Gault equation: eCCr (mL/min/1.73 m2)=(140-age)×weight (kg)/serum creatinine (mg/dL)/72×(0.85 for females)×1.73 m2/body surface area (BSA), and BSA calculated as follows: BSA = weight (kg)0.425 ×height (cm)0.725×0.007184 (9).
CCTA protocols
All CCTAs were obtained using 16-slice (18.4%) or 64-slice (81.6%) CT scanners (Somatom Definition; Siemens Medical Solutions, Forchheim, Germany and Brilliance 64; Philips, Best, the Netherlands). Details of CT scan protocol have been described in previous studies (1011). Before CCTA, all patients with an average heart rate of >65 beats/min received oral metoprolol 50-100 mg in the absence of contraindications, and were given sublingual nitroglycerin 0.2-0.6 mg immediately before scanning. During image acquisition, 60-80 mL of contrast was injected, followed by a saline flush. Helical scan data was obtained using the retrospective ECG-gating protocol. Image acquisition was prescribed to include the coronary arteries, left ventricle and proximal ascending aorta. All CCTA results were transferred to an external three dimensional workstation, and analyzed independently by two experienced radiologists. Coronary atherosclerotic lesions were classified by severity of luminal stenosis, graded as no CAD (0% luminal stenosis) and non-obstructive CAD (1%-49% stenosis) and obstructive CAD (≥50% stenosis). Patient-based analysis was performed.
Clinical events
The primary clinical endpoint was time to composite events consisting of cardiac death, non-fatal MI, unstable angina and late (≥90 days after CCTA) revascularization. Secondary clinical endpoint was time to composite of hard cardiac events consisting of cardiac death and non-fatal MI. Patients with stable clinical features undergoing an early elective revascularization within 90 days after CCTA were excluded from survival analysis (1213). Patient follow-up data were gathered by two observers blinded to the results of CCTA using hospital records or standardized telephone interviews for patients with a follow-up loss of more than recent six months. If a patient could not be reached even by a phone, information on death was obtained from the Korean Ministry of Public Administration and Security. Cause of death was identified. Cardiac death was defined as death in the setting of MI, ventricular arrhythmia, decompensated heart failure or cardiogenic shock. Sudden unexplained death was also considered as cardiac death. Noncardiac death was death not related to cardiac disease. MI was defined based on the following criteria: typical chest pain, elevated cardiac enzyme levels, and typical changes in electrocardiogram (ECG) (14). Unstable angina was defined as acute chest pain regardless of the presence of ECG abnormalities, and negative cardiac enzyme levels (14). The first event was considered as the event of the patient. When two or more events were recorded at the same day, the most serious event was considered as the event of the patient in the following order: cardiac death, non-fatal MI, unstable angina and revascularization.
Statistical analysis
Categorical variables are presented as frequencies with percentages and continuous variables are presented as mean±standard deviation. Categorical variables are evaluated using the chi-square test and continuous variables are evaluated using a Student's t-test. Cox proportional hazards analysis was used to assess predictors of clinical events. Age, sex, body mass index (BMI), smoking status, diabetes mellitus and hypertension considered as confounders should be adjusted. The event rates according to the eCCr, categorized as ≥90 mL/min/1.73 m2, 60-89 mL/min/1.73 m2 and <60 mL/min/1.73 m2, was estimated by the chi-square test of linear by linear association. To assess the cut-off value of eCCr as a predictor of events, receiver operating characteristic (ROC) curve analysis was used. Cumulative event free survival was assessed using the Kaplan-Meier method and compared using the log-rank test. A two tailed P value of <0.05 was considered statistically significant. All data were analyzed using SPSS for Windows 18.0 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics of study subjects
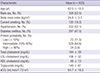
Baseline clinical characteristics of study subjects are shown in Table 1. Their mean age was 62.5±10.3 yr (range, 25 to 85 yr) and 52.5% of the patients were male. About a half of patients had hypertension (53.1%) and diabetes mellitus (47.5%). Most of patients (84.6%) had intermediate pretest probability of CAD. Mean eCCr was 64.7±18.5 mL/min/1.73 m2.
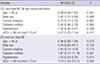
Clinical parameters predicting events
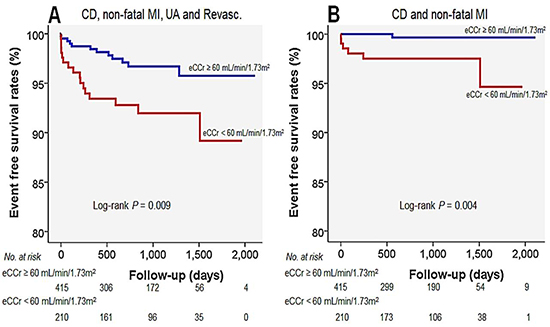
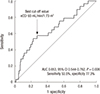
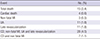
Cardiovascular events were evaluated during follow-up period of 819±529 days (median 837 days). There were four cases of cardiac death (0.6%), three cases of non-fatal MI (0.5%), 11 cases of unstable angina (1.8%) and 11 cases of late revascularization (1.8%). Primary composite events including cardiac death, non-fatal MI, unstable angina and late revascularization occurred in 28 patients (4.5%), and composite hard events including cardiac death and non-fatal MI occurred in seven patients (1.1%). Annualized all- and hard-event rates were 2.00% and 0.49%, respectively. Fifteen patients (2.4%) were died, and mean annualized death rate was 1.06% (Table 2). Clinical parameters predicting cardiovascular events were assessed using multivariable Cox regression analyses (Table 3). Independent predictors for primary composite cardiac events were male sex (hazard ratio [HR], 2.40; 95% confidence interval [CI], 1.01-5.69; P=0.046) and low eCCr (<60 mL/min/1.73 m2) (HR, 3.07; 95% CI, 1.22-7.74; P=0.017). Diabetes mellitus had a marginal significance in this model (P=0.060). eCCr was the only independent predictor for secondary composite hard events (HR, 17.6; 95% CI, 1.44-215.7; P=0.025). Primary composite event rates proportionally increased with decrease of eCCr: event rates were 1.3%, 3.2≥, and 7.6% in subjects with eCCr ≥90 mL/min/1.73 m2, 60-89 mL/min/1.73 m2 and <60 mL/min/1.73 m2, respectively (P=0.006) (Fig. 1). In ROC curve analysis, the sensitivity and specificity for detection of primary composite cardiac events were 53.5% and 77.3%, respectively with eCCr 60 mL/min/1.73 m2 as the best cut-off value (Fig. 2). In Kaplan-Meier survival curve, cumulative primary and secondary composite event free survival rates were significantly lower in patients with low eCCr (<60 mL/min/1.73 m2) compared to those with high eCCr (≥60 mL/min/1.73 m2) (log-rank P<0.05 for each) (Fig. 3).
DISCUSSION
The present study demonstrated that rate of cardiovascular events including cardiac death, non-fatal MI, unstable angina and late revascularization was 4.5%, and cardiac death and non-fatal MI was 1.1% during follow-up period of 819±529 days (median 837 days) in patients without significant CAD on CCTA. The renal function assessed by eCCr was an independent predictor of adverse cardiovascular events in this population. To the best of our knowledge, this is the first report showing the prognostic significance of renal function among patients without significant CAD. The results of the present study suggest that careful monitoring and preventive strategy is necessary for individuals with renal impairment even without significant CAD.
It has been reported that annualized cardiovascular event rate is much lower in individuals without obstructive CAD than those with by CCTA. Min et al. (4) demonstrated favorable outcomes with a 0.22% annualized death rate in patients without CAD. Chow and colleagues showed that annual cardiovascular rates were 0.26% for patients with no CAD, 0.87% for those with non-obstructive CAD, and 4.61% for those with obstructive CAD on CCTA (15). Russo et al. (16) reported excellent prognosis in patients with normal coronary artery with an annualized incidence rate of 0.88% and in patients with mild CAD with 3.89%. Lin et al. (17) demonstrated that individuals with no CAD on CCTA had a favorable intermediate-term prognosis with annualized mortality rate 0.34%. In a meta-analysis, the annualized event rate was 11.9% among patients with insignificant CAD and 0.4% for those without CAD on CCTA (18). Our study results are in line with these previous results showing that annualized all- and hard-event rates were 2.00% and 0.49%, respectively.
Compared to obstructive CAD, the prognostic factors in patients with insignificant CAD evaluated by CCTA has not been well studied. Recently, there was a report investigating 2,583 patients with non-obstructive CAD on CCTA (17). In that study, traditional risk factors including old age, male sex, hypertension, diabetes mellitus, dyslipidemia and smoking status were independent predictors for cardiovascular events. However, they did not evaluate the prognostic impact of renal function in that study. The present study showed that male sex and impaired renal function were independent predictors in subjects without significant CAD.
Chronic kidney disease (CKD) is an independent risk factor of cardiovascular disease (1920). Greater prevalence of traditional cardiovascular risk factors and uremia associated consequencies such as volume overload, anemia, and oxidative stress have been known to contribute to the poor cardiovascular outcomes (19). However, high rates of sudden cardiac death and coronary events in CKD patients without known CAD or after complete revascularization could not be fully understood by these factors (16182122). In this regard, the important role of non-obstructive vulnerable plaque has been suggested as another mechanism how CKD increases the risk (232425). Wada et al. (26) reported that CKD accelerates the formation of vulnerable plaque and increases the frequency of plaque disruption. Baber et al. (22) characterized coronary atherosclerotic plaque morphology in CKD patients using intravascular ultrasound and demonstrated that CKD patients have plaque composed of greater necrotic core and less fibrous tissue prone to rupture. Similarly, Hayano et al. (27) demonstrated that impaired renal function was related to higher percentage of lipid volume within the neointima after stent implantation leading to an increased risk of late stent failure. In addition, it has been reported that impaired renal function causes decreased number of smooth muscle cells within the plaque that may cause loss of fibrous cap of plaque (28). Other studies showed that CKD enhanced carotid artery calcification and reduced collagenous plaque that may lead to plaque instability and rupture (2930).
Besides retrospective design, this study has several limitations. First, we could not provide information on plaque composition or nature that might suggest the clue explaining the high event rates in patients with renal impairment. Second, information regarding management following CCTA was not available. Medications such as aspirin or statin and life style changes might affect clinical outcomes. Also, information on type of medical treatment in patients with diabetes was missing in our study.
The present study shows that renal function is an independent predictor for cardiovascular events among patients without significant CAD by CCTA, and suggests that careful monitoring and preventive strategy are warranted in patients with impaired renal function even without significant CAD.


 XML Download
XML Download