

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pregnancy and childbirth is an important event in a woman's life, regardless of them carrying or not carrying disability. Women with disability are confronted with different circumstances compared to women without disabilities in the case of pregnancy and childbirth. They are faced with problems with disability in itself, and they could be faced with further barriers such as physical accessibility, additional economic burden, problems of communication with medical personnel and sociocultural prejudice (1, 2, 3). Therefore, more delicate care and attention from families, society, and the nation are needed for pregnant women with disabilities. Nevertheless, in Korea, it has not been revealed how many pregnancies and deliveries among disabled women have occurred annually. Although the Korean government surveys nationwide every 3 yr to grasp the status of people with disabilities, this survey only questions how many disabled women have experienced pregnancy (4). Consequently, it has not been revealed how many pregnancies and deliveries among disabled women have occurred annually. There are also insufficient researches in other countries on the nature of disabled women and rates of childbirth, as they only focused on some parts of regions in the country and some types of disability (5, 6, 7, 8). Thus, the first thing we have to do is seize the full-scale of pregnancy and deliveries among disabled women. On the other hand, it is also important to provide prenatal care in pregnancy and delivery to reduce maternal mortality and morbidity, and to early detect problems in the fetus (9). If inappropriate prenatal care is provided to pregnant women, it may result in the following problems; abortion, stillbirth, perinatal death, immaturity, and congenital malformations (9, 10, 11, 12, 13, 14, 15). However there is a rare study regarding the topic on the appropriateness of prenatal care for pregnant women with disabilities.
For these reasons, the aim of this study was to investigate the whole picture regarding pregnancy and delivery among disabled pregnant women using the data of National Health Insurance Corporation (NHIC) in Korea. This includes the following topics; how many disabled women are giving birth, how and where they are delivering, whether they are being given appropriate prenatal care, factors affecting inappropriate prenatal care, and common obstetrical complications they face compared to non-disabled women.
MATERIALS AND METHODS
Materials
The study subjects were selected from the NHIC database, women who terminated pregnancy including delivery and abortion from January 1, 2010 to December 31, 2010. The definition of delivery and abortion was based on the International Classification of Diseases-10th Revision (ICD-10) (Table 1). The types of delivery were divided into cesarean section and vaginal delivery. The outcome of delivery was separated by live birth and stillbirth. The final subjects of this study were 463,847 and 2,968 women of them were classified with disabilities (0.6%).
In this study, the disable woman refers to a female who registered to Korean government as a person with disabilities. Korean government has categorized as 15 types of disabilities such as 6 external impairments (impairment of extremity, stroke & brain injury, visual impairment, auditory impairment, lingual impairment, and facial deformity), 6 internal impairments (kidney, heart, liver, lung, intestine & bladder, and epilepsy), and 3 mental disabilities (mental retardation, mental disorder, and autistic spectrum disorder) (4).
To evaluate the adequacy of prenatal care, we adopted the Kessner Index (16). Depending on the total number of visits for prenatal care, if the total number of visits were more than 9, it would be evaluated as 'adequate', if visited 5-8 times 'intermediate', and if they visited less than 4 times it would be 'inadequate'. Using the ICD-10 code, obstetrical complications were operationally defined into preeclampsia (O14), eclampsia (O15), gestational hypertension (O13), gestational diabetes mellitus (O244), placenta previa (O44), abruptio placentae (O45), obstructed labor (O64-O66), and preterm delivery (O601) (Table 1). Also, we used not only primary diagnostic code but also the first recorded secondary diagnostic codes (1 primary code and 1 secondary code). We used the national health insurance premium as a proxy indicator of the level of income. It was categorized as three levels; high level (upper 25% of premium), intermediate level (middle 50%), and low level (lower 25%). In addition, Severity of disability was divided into "severe (grade 1-3)" and "mild (grade 4-6)" by their disability grades.
Statistical analysis
Frequency analyses were conducted to describe the full-scale of pregnancy and delivery among disabled women in Korea. We conducted Pearson's chi-square test and Student-t test to examine the difference between disabled women and non-disabled women. To define the factors affecting inadequate prenatal care, multivariate analysis was performed using logistic regression method. All the analyses were completed using SPSS, version 19.0 (IBM, Chicago, IL, USA). All statistical tests were two-sided and a P value <0.05 was considered statistically significant.
RESULTS
General characteristics of subjects
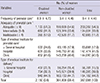
In 2010, the total number of pregnancy were 463,847. Of them, 2,968 (0.6%) cases were from disabled women and 460,879 (99.4%) cases were from non-disabled women. It was more likely for disabled women to be pregnant in the over 35 age group (36.4%) compared to non-disabled women (23.2%) (P < 0.001). Disabled women tended to live in rural areas (11.5%) compared to non-disabled women (8.1%) and beneficiaries of Medical Aid in disabled women were higher (12.8%) than in non-disabled women (0.9%) (P < 0.001). Also, the rate of low level of income were higher in disabled women (43.6%) than non-disabled women (25.2%) (P < 0.001). Over 60% of disabled women had mild type of disability (Table 2).
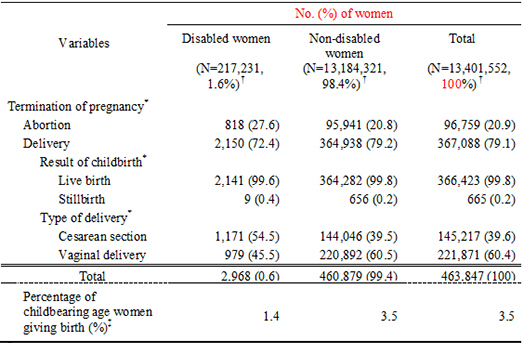
The full-scale of abortion and delivery, and type of delivery
As of 2010, there were 13,401,552 women in the childbearing age in Korea. Out of these, there were 217,231 (1.6%) disabled women and 13,184,321 (98.4%) non-disabled women. There are two types of termination of pregnancy, which are delivery and abortion. In the case of disabled women, the percentage of childbearing age women giving birth was 1.4%, which was significantly lower than non-disabled women (3.5%) (P < 0.001). Abortion rates were statistically significant with 27.6% of disabled women and 20.8% of non-disabled women (P < 0.001). The number of disabled women undergoing the Cesarean section was also statistically significant as 54.5% delivered through the procedure, in comparison to 39.5% of non-disabled women (P < 0.001) (Table 3).
Adequacy of prenatal care, place of prenatal care, and delivery
During the whole pregnancy period, disabled women received 8.9 occasions of prenatal care while non-disabled women received it on 9.4 occasions: thus disabled women receiving it 0.5 occasions less. Disabled women receiving inadequate prenatal care was significantly higher (17.0%) than non-disabled women (11.7%). A higher rate of disabled women utilized general hospitals for prenatal care and delivery services (P <0.001) (Table 4).
Factors affecting inadequate prenatal care
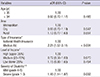
To define the factors affecting inadequate prenatal care, we conducted logistic regression for adjusting the effect of variables (age group, area, type of insurance, level of income, and severity of disability). The results showed that beneficiaries of Medical Aid were 2.21 times more likely to receive inadequate prenatal care (P < 0.001). Compared to mild disabled women, severe disabled women were 1.46 times more likely to receive inadequate prenatal care (P = 0.002) (Table 5).
Obstetrical complications
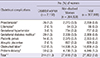
In regards to the eight obstetrical complications we operationally defined in this study, 11.3% of disabled women experienced at least one complication, which was higher than non-disabled women with 7.6% (P < 0.001). In detail, preeclampsia (P = 0.001), gestational diabetes mellitus (P < 0.001), obstructed labor (P < 0.001), and preterm delivery (P < 0.001) were statistically higher in disabled women than non-disabled women (Table 6).
DISCUSSION
Disabled pregnant women may be more vulnerable than non-disabled pregnant women therefore more delicate care and attention is needed. However there is rare evidence or research performed on this subject and there is even no information on the full-scale of the number of pregnancy and delivery among disabled pregnant women annually based. From this point, this study can be providing meaningful information not only to the Korean society but also to the international society. Through this research, we found out how many disabled women were giving birth, where and how they were delivering, common obstetrical complications they faced, whether they were being given appropriate prenatal care, and factors affecting inadequate prenatal care.
According to a report conducted by the Korean government, disabled women got married earlier than non-disabled women however the age of pregnancy among disabled women were higher in the age group of 35 or older than non-disabled women (17). Medically, women who experience pregnancy at aged 35 and over are in danger of high-risk pregnancy (18, 19). Our results also showed that the proportion of disabled women in the 35 or over age group were higher than that of non-disabled women. Although the reasons behind this have not been revealed in this study, disabled women in the high-risk pregnancy in terms of age are in need of more delicate care. We should consider the possibility of geographical, economical, and physical barriers in pregnant disabled women. According to our results, in contrast to non-disabled women, a higher number of pregnant disabled women were residing in rural areas, requiring beneficiaries of Medical Aid, and receiving low income. Non-disabled women have no physical barriers however disabled women carry these barriers already exist within themselves.
In 2010, there were 2,968 pregnancies terminated from disabled mothers, which is a proportion of 0.6% out of the total numbers of pregnancies terminated. However the proportion of childbearing aged women was 1.6% of disabled women and 98.4% of non-disabled women. Therefore, in proportion, disabled women's termination of pregnancy is lower than non-disabled women. In addition, the rate of disabled women childbearing age (15-49 yr) giving birth was 1.4%, which was lower than 3.5% in non-disabled women (P < 0.001). In sum, disabled women giving birth are low in the absolute number and low in proportion compared to non-disabled women. This could be a result from disabled women avoiding giving birth (4).
Interestingly, abortion rates among disabled women (27.6%) were higher than non-disabled women (20.8%) (P < 0.001). The reasons might be due to the vulnerable health status of disabled mothers (i.e., miscarriages) or it could be from following the advice of close people around them to abort the pregnancy. It could also be possible that disabled mothers were pressured from the social stigma or discrimination of them giving birth (4, 20). However, this research cannot reveal the reasons behind these two differences therefore further research should be undertaken. Regarding delivery methods, the rate of Cesarean section among disabled women (54.5%) were higher than non-disabled women (39.5%) (P < 0.001). The reasons might be explained as such; there may be cases where the Cesarean section is medically needed due to the health status of disabled women, or the mother and/or family may favor the Cesarean section rather than going through the labor pain, and finally the doctor may also prefer the Cesarean section to reduce any risks for the disabled mother.
This research has revealed that a high number of disabled women utilized high level healthcare organizations such as general hospitals for prenatal care and giving birth than non-disabled women (P < 0.001). In general, when pregnant women use general hospitals for prenatal care and delivery services, it can mean they are in the high-risk pregnancy or they should be cared with more delicate services. In respect to this point of view, the results of this research can be understood. Nonetheless, the possibilities cannot be excluded; disabled pregnant women themselves and/or family could desire them to utilize general hospitals; or doctors may prefer to refer these women to general hospital to avoid any risks to mother and/or baby.
Have these pregnant disabled women received appropriate prenatal care? In order to evaluate the appropriateness of prenatal care, we adopted the Kessner Index (16). According to this index, if a pregnant woman had less than 4 visits to the doctor for prenatal care, this would be evaluated as inadequate. The rates of inadequate prenatal care in disabled women (17.0%) were higher than non-disabled women (11.7%). The average frequency of prenatal care was also lower in disabled women (8.9 occasions) than non-disabled women (9.4 occasions) (P < 0.001). What factors affected the inadequate prenatal care among disabled women? That is, asking why some disabled mothers utilized prenatal care on less than 4 occasions. Disabled mothers receiving inadequate prenatal care can be harmful to both mother and baby; and such reasons can be affected to the fact; there may have been limitations to accessibility from physical barriers and/or economic burden. To define this, we adopted the logistic regression for adjusting the variables. Our results showed that beneficiaries of Medical Aid and mothers with severe disability were likely to receive less prenatal care than 4 occasions. In short, economic and physical barriers were statistically significant factors affecting inadequate prenatal care.
Ideally, during the pregnancy period, any obstetrical complications should be prevented, but if impossible, it should be minimized. Our results show that obstetrical complications in disabled women are higher in comparison to non-disabled women. These women are in a vulnerable state therefore suffering more. It means that they need more attention and delicate healthcare services. Therefore, adequate prenatal care is essential for disabled women to detect any obstetrical complications at an early stage and to also appropriately manage them.
There are some limitations and further research subjects in this study. Firstly, to decide inadequate prenatal care we adopted the Kessner Index (16), and indicated the term 'inadequate' when there were less than 4 prenatal care visits. Thus this could be limited to the study only evaluating the quantity of visits and not the quality of care received. Secondly, some essential health outcomes on babies from disabled women such as neonatal weight, congenital anomalies, and infant mortality could not be examined due to privacy limitations from legal reasons. Thirdly, to investigate the nature of pregnancy, prenatal care and delivery of disabled women we only compared disabled women and non-disabled women as a whole. Therefore further detailed research should be undertaken in order to reveal information which were not undertaken in this study. For example, why there are a higher number of aged 35 or over disabled women experiencing pregnancy, the real reason behind disabled women's abortion, the types of pressure disabled women undergo while pregnant, and why they opt for Cesarean section. Lastly, to calculate the prevalence of preterm labor, we only used O601 (preterm spontaneous labor with preterm delivery) instead of using O60 (O601, O601, O602, and O603) (Table 1). Therefore, in this study, the prevalence rate of preterm labor (1.3%) is lower than in case of using O60.
Nevertheless, our study provides meaningful information to the Korean government and international society. To our knowledge, our study is the first study using the National Health Insurance Data for investigating the whole picture regarding pregnancy and delivery among disabled pregnant women in Korea.
From our study, we were able to discover that disabled women were more vulnerable in pregnancy, prenatal care and delivery. Therefore, the government and society should pay more attention to disabled pregnant women to ensure they have a safe pregnancy period up until the delivery. This should be done to prevent or minimize any obstetrical complications and to guarantee the health of both mother and baby. The government can consider starting a pilot study as a form of demonstration program for pregnant women with disabilities like "The Supporting Program for Obstetric Care Underserved Areas (SPOU)" (21). From this point, our study can be the first step for the government and society to understand what should be provided and attended to for disabled pregnant women.
 XML Download
XML Download