

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hypercholesterolemia is a well-established risk factor for cardiovascular disease (CVD), and accounts for 4.5% of all-cause mortality worldwide (1). Furthermore, it is a risk factor that can be modified by therapeutic lifestyle changes (TLC) and lipid-lowering agents (23). Among the available lipid-lowering therapies, statins represent a cost-effective tool for the primary prevention of coronary heart disease (45), and can reduce the relative risk of major vascular events by 20% for each 1 mM/L reduction in low density lipoprotein (LDL) (6).
The National Cholesterol Expert Panel (NCEP) recommends screening for dyslipidemia in individuals from the age of 20 yr and initiating lipid-lowering medication in cases where the therapeutic goal is not reached within 12 weeks of TLC. The United States Preventive Services Task Force (USPSTF) and European Society of Cardiology (ESC) similarly support screening and therapeutic intervention for dyslipidemia. Based on these recommendations, many countries are conducting national screening programs for dyslipidemia, including Japan, Korea, United Kingdom, and the United States. In Korea, the National Health Insurance Corporation (NHIC) introduced an examination for hypercholesterolemia in the biennial National Health Screening Program (NHSP) in 1995.
However, previous studies have shown that the invitation of patients for health checks failed to improve total mortality or cardiovascular mortality (7), and that for a screening program to be effective in clinical settings, appropriate therapeutic interventions should be employed (8). In usual medical practice, compliance of patients following the prescription of lipid-lowering therapy is known to be poor (9). However, only few empirical studies have investigated the follow-up practices after population screening regarding appropriate prescription of lipid lowering agents when patients are detected with hypercholesterolemia.
The number of statin prescriptions written can be a strong surrogate marker of effective clinical intervention for hypercholesterolemia, because statins are the most frequently prescribed (87%) lipid-lowering agents (10). Therefore, we analyzed the statin prescription rate for newly diagnosed hypercholesterolemia and sustained hypercholesterolemia patients identified by the national screening program as the primary outcome. We also analyzed factors associated with statin prescription rates, to examine the patients at risk of not receiving effective treatment in spite of having sustained hypercholesterolemia.
MATERIALS AND METHODS
NHSP in Korea
Screening for hypercholesterolemia is a part of the NHSP. The NHSP is a population-based health-screening program provided biennially by the Korean NHIC, a universal healthcare payer covering nearly the whole Korean population (96.9%). The participation rate in the NHSP was 48% in 2003 and increased to 73% in 2011. The NHIC directly invites the subjects to participate in the program and afterwards informs them about the test results. During the process, subjects are to choose for themselves which medical center or clinic they wish to get their screening tests done and receive the necessitated management from.
Data sources
This study is based on the insurance registry database of NHIC members, their NHSP data, and the Korean National Health Insurance (NHI) medical service claims data. The NHSP data provided information about serum cholesterol levels and health behaviors. The NHI medical service claims data provided information on medical history, including comorbid diseases and statin prescriptions.
Study subjects
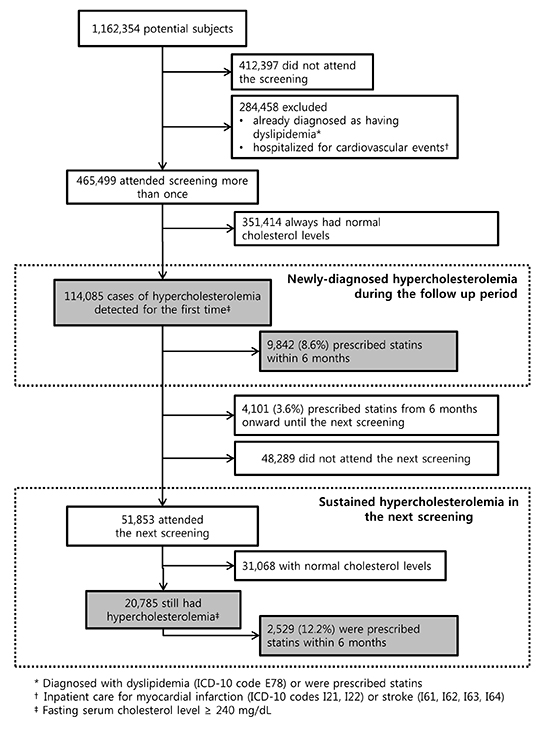
The potentially eligible subjects included 3% of the adults (>20 yr) who were selected randomly from the NHIC registry, as of December 31, 2002. They included 3% random sample of householders stratified by age and gender using the social security number and their household members. The follow-up period was up to 8 yr, through December 31, 2010. Among 1,162,354 eligible subjects, we excluded 412,397 subjects who did not participate in the screening program during the study period. We also excluded 284,458 subjects who were diagnosed with hypercholesterolemia, prescribed statins, or hospitalized for myocardial infarction (ICD-10 codes I21, I22) or stroke (I61, I62, I63, I64) before they first attended the NHSP. The number of subjects in the study population was 465,499 (Fig. 1).
Definitions and study outcome
Newly diagnosed hypercholesterolemia was considered when cases of hypercholesterolemia were diagnosed for the first time during the study period. Sustained hypercholesterolemia was defined as those with hypercholesterolemia in >2 consecutive screenings, each in 2 yr interval. To evaluate the clinical intervention rate in the NHSP strictly, we operationally defined the target population for statin treatment as cases with sustained hypercholesterolemia on the consecutive screening after the first diagnosis (newly diagnosed hypercholesterolemia) (Table 1). Hypercholesterolemia was defined as a total serum cholesterol concentration of ≥6.2 mM/L (≥240 mg/dL) (4). Serum cholesterol was tested in fasting conditions, and the level was measured using an enzymatic method. Quality control in each hospital was assured by the Korean Association of Laboratory Quality Control (11).
Statin prescription was defined as the prescription of statins within 6 months after detection through the NHSP. The time limit of 6 months was set to measure the direct effect of NHSP, while considering the 12 weeks of TLS in the NCEP recommendation (4) as well as a cushion period. The prescription code included any form of statin listed in the claims data: atorvastatin, fluvastatin, pitavastatin, pravastatin, rosuvastatin, and simvastatin. Based on these definitions, we analyzed the statin prescription rate for newly diagnosed hypercholesterolemia and sustained hypercholesterolemia patients as the primary outcome measure.
Statistical analyses
Descriptive statistics were used to present data on the attendance for health-screening check-ups as well as statin prescription information. Among clinical characteristics of study subjects, Charlson comorbidity index (12) was calculated using the diagnosis for inpatient care from the KNHI medical service claims data. To evaluate the correlation between subject characteristics and statin prescription, a multivariate logistic model was constructed based on the univariate analyses of risk factors of coronary heart disease (CHD) (4) using the stepwise selection technique. In the final model, we calculated the odds ratio and 95% confidence intervals, adjusted for gender, age, comorbidities (hypertension and diabetes), smoking, and year of examination. We used STATA version 12.0 (StatCorp. Houston, TX, USA) to analyze the data, and the statistical significance was defined as P<0.05.
RESULTS
Diagnosis of hypercholesterolemia and statin prescriptions
Among 465,499 subjects who attended the first screening visit of the NHSP and were not previously diagnosed with hypercholesterolemia, 114,085 subjects (24.5%) were newly diagnosed with hypercholesterolemia. Of these, 8.6% (n=9,842) were prescribed with statin within 6 months of the NHSP, and an additional 3.6% (n=4,101) were prescribed statins in the subsequent 6 months until the next NHSP screening.
Among the 100,142 subjects who had not been prescribed for a statin after their initial diagnosis of hypercholesterolemia, 51,853 (51.8%) attended the next NHSP screening and 20,785 of these subjects (40.1%) had sustained hypercholesterolemia. However, only 12.2% (n=2,529) of them were prescribed statin treatment within 6 months following the examination (Fig. 1).
Statin prescription after hypercholesterolemia by age, sex, and comorbidities
The statin prescription rate was higher among women than men for those aged ≥40 yr; this trend was not observed for those aged <40 yr. Considering CVD risk factors, people were prescribed statins more frequently if they were diagnosed as hypertension and aged from 20 to 59 yr old. Notably, male patients of all ages and female patients aged >40 yr, who had been diagnosed with diabetes, were most frequently prescribed with statins. The prescription rate was high in subjects with sustained hypercholesterolemia compared to subjects with newly diagnosed hypercholesterolemia regardless of gender or age (Table 2).
Factors associated with statin prescriptions in subjects with sustained hypercholesterolemia
Among 20,785 cases of sustained hypercholesterolemia, statin prescriptions correlated with female gender (adjusted odds ratio [aOR], 1.73; 95% CI, 1.40-2.15) and older age (aOR for age 40-59 yr, 2.13; 95% CI, 1.73-2.63; aOR for ages 60-79 yr, 2.55; 95% CI, 1.94-3.34). Past diagnoses of comorbidities were also important correlates, including hypertension (aOR, 1.41; 95% CI, 1.19-1.67) and diabetes (aOR, 1.26; 95% CI, 1.00-1.34). Above all, statin prescription rates were found to have increased in recent years (aOR for 2007-2008, 1.27; 95% CI, 1.13-1.43; aOR for 2009-2010, 1.70; 95% CI, 1.53-1.89) (Table 3).
DISCUSSION
To our knowledge, this is the first longitudinal report about the treatment gap observed in a population-based dyslipidemia screening program. It is an important issue because it could limit the full benefit of a prevention program for cardiovascular diseases (13). The strengths of our study include the use of a large database from a nationally representative sample, and the nearly complete follow-up for the primary outcome variable. The use of claim data for comorbidities and statin prescription details, rather than self-reported information, is another strength compared to other previous studies reporting prescription rates for dyslipidemia (141516).
Although we designed a conservative study, only 12.2% of patients with sustained hypercholesterolemia were prescribed with statins within 6 months of the screening. This suggests that many patients with hypercholesterolemia do not receive appropriate clinical intervention despite their active participation in a consecutive health-screening program, indicating that the test results may not be suitably utilized for preventing CVD. Participants were more likely to be prescribed statins if they had established risk factors (4). This was the case if they were older, hypertensive, diabetic or middle-aged and older women. However, the prescription rates were <20% even for higher risk groups, such as older people, smokers, and those with diabetes or hypertension, although recent guidelines have recommended intensive statin treatment in such high risk groups (4).
Although the data may not be directly comparable, our results are in marked contrast to the statin prescription rates seen in the National Health Service (NHS) Health Check in the UK. In the first 2 yr of the NHS Health Check, statin prescription rates increased from 14.0% to 60.6% between the pre- and post-screening periods in groups at high risk of CVD (17). The discrepancy in the efficacy of NHS Health Check and NHSP could be due to the different degree of integration and the continuity of healthcare services. In the NHS Health Checks, the test is ordered and followed up by medical professionals who care for each patient at high risk (18). The cardiovascular disease screening by Medicare in the US adopts a similar process where the test is initiated by doctors or healthcare providers for their own patients (19). However, the NHSP is operated independently from the primary care physicians of individual patients. Physicians cannot browse nor follow up on the NHSP reports for their patients. In the NHSP, patients have to apply for the screening, receive the test report, and then seek medical advice by themselves.
Compliance with lipid-lowering therapy is usually poor (9). It has been reported that many patients were not concerned regarding their cholesterol level reports (20), were not aware of the desirable cholesterol levels (2122), or did not understand its importance as a risk factor for CVD (2223). In addition, patients often believe that TLC would be equally as effective at lowering cholesterol as statins (20) and often have concerns about the adverse effects of statins (202425). Therefore, it is difficult to achieve appropriate treatment if the clinical follow up is left entirely to the patient. A promising finding was that the prescription rate increased from 10.0% to 15.5% during the study period of 8 yr. This finding agrees with the increasing trend of lipid-lowering drug use worldwide (5141526), although the prescription rate is still low in Korea, as reported in 2011 (27).
This study has several limitations. First, our study evaluated only the treatment gap in the NHSP. During the study period (median follow-up, 3.86 yr), we could not assess for a significant decrease in myocardial infarction and all-cause mortality using information on statin prescription within the first 6 months (data not shown). The effect of pharmacologic intervention rates on long-term clinical outcomes in every stage, such as the treatment rate, control rate, cardiovascular event, and cardiovascular mortality remains to be investigated. Second, in the present study, the criteria for statin prescriptions were based on serum total cholesterol level only, and not on the LDL or High Density Lipoprotein (HDL) levels that are used in clinical practice. In Korea, serum total cholesterol levels have been used as the conventional standard for prescribing statins for a long time (27), and during the study period, the National Health Insurance allowed insurance coverage for statin prescription based on the serum total cholesterol level. In a similar vein, the National Health-Screening Program tested only for serum total cholesterol levels until 2008. Although recent guidelines are focusing more on the LDL or HDL levels, we adopted the conventional standard during the study period for the fair evaluation of the follow-up practice during the same period. Meanwhile, the total cholesterol levels are good for predicting the risk of cardiovascular disease, compared to the new biomarkers (228). Moreover, statin prescription rates were still very low in high risk groups, suggesting that the conclusion of our study would be robust even with different criteria for statin treatment. Third, a comprehensive evaluation of interventions for dyslipidemia was not considered, as we had no information on the TLC. However, we overcame this limitation by using the criterion of statin prescription only in patients with sustained hypercholesterolemia. Fourth, the statin prescription rate may have been overestimated due to a selection bias, as participants in a health-screening program are more likely to be interested in their health and adhere to clinical follow-up.
In spite of these limitations, this study showed that a wide treatment gap is present in the NHSP in Korea, although it is improving. There has been remarkable development in lipid-lowering therapies, which can help in cases of sustained dyslipidemia (6). Considering the contrasting findings between NHSP and NHS Health Check, the real-world benefit and efficacy of screening programs can vary widely. Therefore, to reduce the cardiovascular disease burden, it would be worthwhile to decrease the treatment gap and to re-evaluate the clinical benefits of a health-screening program.



 XML Download
XML Download