

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Marfan syndrome (MFS) is an autosomal dominant connective tissue disorder with cardiovascular, skeletal and ocular manifestations (1). The diagnosis of MFS relies on the revised Ghent nosology, which weights cardiovascular manifestations more heavily and in which aortic root aneurysm and ectopia lentis are the cardinal clinical features (23). In the revised Ghent nosology, the most selective systemic features were included in the systemic score and each element was assigned one, two, or three points based on its importance to diagnosis (2). Protrusio acetabuli (PA) was assigned two points, as was dural ectasia, spontaneous pneumothorax, anterior chest deformity, and hindfoot deformity (2).
PA has various etiologies, including infectious, neoplastic, inflammatory, metabolic, traumatic, and genetic causes (4). There are a few methods to diagnose PA using plain anteroposterior radiographs of the pelvis. The prevalence of PA, which is different according to the diagnostic method, is 23%-46% in Korean MFS patients and 16%-100% in Western countries (56789). The three most widely used criteria are the Steel method (using a center-edge angle of Wiberg >50°), the Armbuster method (an acetabular-ilioischial distance of ≥3 mm in male patients or ≥6 mm in female patients), and crossing of the teardrop figure (Fig. 1) (51011). Some consider the Armbuster method the most reliable measurement of PA, but other studies have reported that plain radiographic measurements of PA become unreliable as pelvic tilt increases (1112).
In MFS, computed tomography (CT) angiography is commonly performed to investigate the abnormality of aorta. In the axial view, the loss of the normal oval shape of the pelvic inlet at the level of the acetabulum can be easily identified and is considered a sign of PA. A new CT-based diagnostic criterion was recently introduced and the degree of PA could be measured using this method (13).
Some skeletal manifestations of MFS have been known to be associated with other skeletal manifestations or the severity of aortic root dilatation (1415). One study reported that dural ectasia was related to skeletal manifestations and aortic Z-scores (14). However, PA has not been evaluated to correlate with other skeletal manifestations of MFS or aortic root dilatation.
Therefore, we investigated the prevalence of PA using the CT-based diagnostic method in Korean patients with MFS, the association of PA with other manifestations of MFS, and contribution of PA to MFS diagnosis.
MATERIALS AND METHODS
Study population
We reviewed data that was entered into our Marfan database between March 2006 and September 2013. Total 154 patients ≥18 yr of age with a FBN1 mutation were identified. Eight patients who did not undergo CT examination due to renal dysfunction and contrast allergy were excluded. All 146 patients fulfilled MFS diagnostic criteria by the revised Ghent nosology.
Revised Ghent nosology
In the revised Ghent nosology, cardiovascular manifestations are more heavily weighted and aortic root aneurysm and ectopia lentis are the cardinal clinical features. In the absence of any family history, the presence of these two manifestations is sufficient for diagnosis of MFS. In the absence of either of the cardinal clinical features, the presence of a FBN1 mutation or a combination of systemic score is required (Table 1).
Control population
The control cases were selected from patients who visited the emergency room between July 2007 and December 2013 and underwent abdominal and/or pelvic CT, and were age- and sex-matched to Marfan patients. Control candidates with hip joint problems or any known connective tissue disease were excluded from this study.
CT image
Multidetector computed tomography (MDCT) was performed using a dual-source CT scanner (Definition Flash; Siemens Healthcare, Forchheim, Germany) with 2×64×0.6 mm collimation, section acquisition of 2×64×0.6 mm, and z-flying focal spot technique in both the study and control populations. The scanning parameters were 100 kV, 200 mA with automatic tube current modulation (Caredose 4D; Siemens Healthcare), a pitch of 1.0-1.2 and a 0.28-sec tube rotation time.
Measurements and definitions
PA was assessed quantitatively by the CT-based circle-wall distance (CWD) method (Fig. 1). This method uses axial CT images and was introduced by Lundby et al. (13) in 2011. In this method, PA was quantified by using a circle with a 10 cm radius. The circle was fitted to the inner pelvic wall at the level of the acetabulum where the cranial border of the superior pubic ramus fuses with the anterior column of the acetabulum. This level usually includes the fovea of the femoral head. The circle was best fitted to the concavities of the inner walls of the anterior and posterior columns of the acetabulum. We then measured the distance between the line of the circle and the medial most point of the inner pelvic wall of the acetabular fossa (CWD). A positive distance indicates that this medial most point is medial to the circle. Increasing degrees of PA have increasing positive values of CWD. A cut-off value of 1.25 mm was used for diagnosis of PA via the CWD method (13).
We divided the systemic scores into a skeletal score, which included all skeletal manifestations, and non-skeletal scores which included pneumothorax, skin striae, myopia >3 diopters, and mitral valve prolapse.
Statistics
Continuous data are expressed as the mean±standard deviation or median and interquartile range. Categorical data are expressed as frequency and percentage. To evaluate differences between the study groups, we used the Student's unpaired t-test for normally distributed data and the Mann-Whitney test for skewed data. Categorical data was analyzed using the chi-square test or Fisher's exact tests by SPSS software (SPSS for Windows, version 20.0, IBM Corp., Armonk, NY, USA).
RESULTS
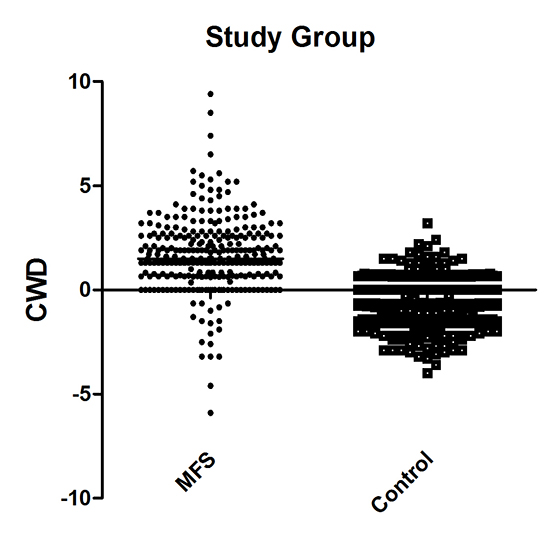
PA was diagnosed in 77.4% of the MFS group and in 11.0% of controls (Table 2). The median CWD was 1.50 mm (range, -5.90 -9.40 mm) in MFS group and -0.64 mm (range, -4.00 -3.20 mm) in controls (P<0.001, Fig. 2).
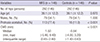
Clinical characteristics of MFS patients according to presence of PA were summarized in Table 3. Of patients with MFS and PA, 45.1% were male; in patients with MFS but without PA, 84.8% were male (P<0.001). The mean height of patients with PA versus those without PA was 176.4 vs. 181.6 cm (P=0.015), mean weight was 66.1 vs. 74.2 kg (P=0.011), mean body mass index (BMI) was 21.2 vs. 22.4 kg/m2 (P=0.069), and median body surface area (BSA) was 1.76 vs. 1.98 m2 (P=0.005), respectively. Hence, anthropometric data showed that patients with PA generally had a smaller body habitus. Important diagnostic criteria, such as a family history of MFS, ectopia lentis, and aortic root diameter, were not significantly different between the two groups (P=0.684, P=0.814, and P=0.062, respectively). Rates of aortic dissection did not differ between the two groups (P=0.333).
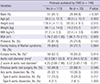
The prevalence of systemic score points ≥7 was more common in the PA-positive group than in the PA-negative group (78.8 vs. 60.6%, P=0.035, Table 4). Median systemic score points were higher in the PA-positive group (10.0 vs. 7.0 points, P<0.001) and median skeletal score points were also higher in the PA-positive group (8.0 vs. 6.0 points, P<0.001). Because the presence of PA is worth 2 points in the calculation of the systemic score, we compared skeletal score points other than PA points. The median skeletal score points excluding PA did not differ between the two groups (6.0 vs. 6.0 points, P=0.322). We analyzed each element of the skeletal score. There was also no association between PA and the elements comprising the skeletal score. However, scoliosis was numerically but not statistically significantly more frequent in the PA-positive group (20.4 vs. 6.1%, P=0.055). The median non-skeletal score points were not significantly different (1 vs. 1 point, P=0.493). CWD was weakly correlated with skeletal score points (P<0.001, correlation coefficient=0.391).
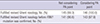
Among 146 patients with FBN1 mutation, only one patient did not fulfill the revised Ghent nosology if the two points attributable to PA were not included (Table 5). In real world clinical practice, genetic diagnosis of FBN1 mutation takes several weeks or months. Therefore, if we assume that we do not know the FBN1 mutation status, three patients would not have met the revised Ghent nosology. If both FBN1 mutation and presence of PA were not included, five patients did not meet the diagnostic criteria for MFS.
DISCUSSION
In the revised Ghent nosology, two points are assigned to the presence of PA in systemic score criteria (2). There are various methods for diagnosing PA, usually using plain anteroposterior radiographs of the pelvis. Of this, the Steel and Armbuster methods were representative. The Steel method uses the center-edge angle of Wiberg, and the Armbuster method uses the acetabular- ilioischial distance. In one study, the prevalence of PA in patients with MFS differed depending on the method used, with 27% of patients considered to have PA using the Steel method and 16% using the Armbuster method (9). Other studies have reported that CT or magnetic resonance imaging (MRI) are going to be more reliable (1112).
In patients with MFS, CT is commonly used to evaluate dilatation, aneurysm, or dissection of the aorta. In PA, a loss of the normal oval shape of the pelvic inlet at the level of the acetabulum is typically noted on axial CT images. Lundby et al. (13) recently introduced a new method to diagnose PA using axial CT images. They measured the distance between the line of the imaginary 10 cm radius circle and the medial most point of the inner pelvic wall of the acetabular fossa. In their study, the exact prevalence of PA by the CWD method was not reported, but was calculated to be 74.7% in Ghent nosology positive patients and 3.7% in controls (13). In our study, the prevalence of PA using the CWD method was similar in the MFS group and more frequent in controls compared to Lundby's study. PA developed more frequently in females and patients with a smaller body habitus.
The CWD method uses a circle with a 10 cm radius to quantify and cut-off value for diagnosis of PA was 1.25 mm. Some study reported that there might be racial and ethnic differences in clinical manifestations between Asian and Western MFS patients (1617). Akutsu et al. (16) reported that major skeletal criteria were less frequent in the Japanese population than the Western population, especially arm span to height ratio >1.05, scoliosis, reduced extension at elbows, and joint hypermobility. Yoo et al. (17) reported that Korean MFS patients less frequently fulfilled major skeletal criteria than Western MFS patients. Therefore, further study is needed to investigate the prevalence of PA between Asian and Western MFS patients, and establish appropriate cut-off value when using the CWD method for diagnosis of PA in Korean MFS patients. However, the absence of a gold standard for PA diagnosis prevents the establishment of an appropriate cut-off value.
MFS has multiple manifestations that may be related to each other. Indeed, PA was known to associate with scoliosis (15). Sheikhzadeh et al. (14) reported that dural ectasia, which adds two points to the systemic score like PA, correlates with aortic Z-scores and skeletal involvement. In our study, aortic root diameter, aortic Z-scores, family history of MFS, and ectopia lentis was not significantly different between the PA-positive and PA-negative groups. Furthermore, PA was neither associated with a history of aortic dissection nor a particular type of aortic dissection. Patients with PA had higher total systemic and skeletal scores than those without PA, but this difference was lost when PA was not included in systemic and skeletal scores. Considering each element of the skeletal score, there was no relationship between each element of the skeletal score and PA, except the higher tendency for scoliosis observed in the MFS group. In the study of Sheikhzadeh et al. (14), they included dural ectasia points in their skeletal score calculation. Therefore, if dural ectasia was not considered in their skeletal score calculation, it might be possible that there was no association between dural ectasia and skeletal score. An other study reported that no association between aortic dilatation and dural ectasia (18).
CT angiography is useful in the diagnosis of other manifestations of MFS in addition to cardiovascular findings. We can evaluate the presence of pectus carinatum or excavatum, scoliosis or thoracolumbar kyphosis, apical blebs, and dural ectasia as well as the presence of PA. Sohn et al. (7) reported that 24% of the study population could be diagnosed with MFS using only CT images. Among our 146 patients, only one patient would not fit criteria for MFS if we excluded the presence of PA. Even though PA does not greatly impact MFS diagnosis, the presence of PA may be helpful for the suspicion of MFS when aortic dissection or aneurysm is found on CT angiography of the aorta.
Our study has several limitations. First, the symptoms and signs of PA were missing in our study. Because of retrospective design of the study, we could not assess how many MFS patients with PA had the symptoms. Second, our MFS patients were unlikely to represent individuals from the general population. Our hospital is a major hospital in Korea, and most patients were referred from other hospitals for surgery for aortic root dilatation or dissection. Accordingly, most of our MFS patients satisfy the aortic Z-score or aortic root dissection criteria, which are essential for the diagnosis of MFS under the revised Ghent nosology. Third, our study did not include patients less than 18 yr of age, because they usually do not undergo CT due to concerns regarding radiation exposure.
In conclusion, even though the presence of PA does not related to the cardinal clinical features of MFS or influence MFS diagnosis, its presence may be helpful for the suspicion of MFS when aortic dissection or aneurysm is found on CT angiography of the aorta because of the high frequency of PA in MFS patients.




 XML Download
XML Download