

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sudden sensorineural hearing loss (SSNHL) is a medical emergency. Therefore, searching for the mechanisms of SSNHL development is very important in establishment of the fundamental therapeutic strategy of SSNHL. However, the exact patho-physiologic mechanism of the sudden sensorineural hearing loss (SSNHL) has remained elusive. It has been suggested that the following factors are causes of SSNHL: idiopathic (71.0%), infectious disease (12.8%), otologic disease (4.7%), trauma (4.2%), vascular or hematologic (2.8%), neoplastic (2.3%), and other causes (2.2%) (1). It is defined as hearing loss of 30 dB or more over at least three contiguous frequencies occurring within 3 days or less (2). Recently, some studies have reported an association between genetic risk factors and SSNHL (345).
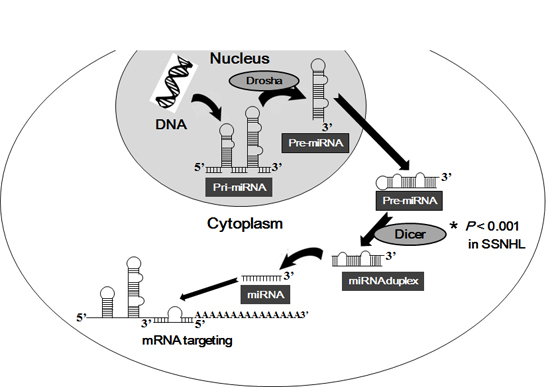
MicroRNAs (miRNAs) are small noncoding RNAs, which are 21-24 nucleotides (nt) in length and play an important role in the post-transcriptional gene regulation by translational inhibition and/or inducing degradation of the target mRNA (6). Many studies reported that miRNAs are involved in a wide range of biological processes such as cellular development, differentiation, proliferation, metabolism, carcinogenesis, and cell death (789). The biogenesis of miRNA occurs in a well-organized process, referred to as the 'miRNA machinery' (10), which is mediated by two important RNAse III endonucleases including Dicer and Drosha (611). Drosha is a part of a multiprotein complex, the DROSHA/DGCR8 miRNA microprocessor and cleaves primary miRNAs (pri-miRNA; a single-stranded RNA extensions consisting of a hairpin stem, a terminal loop, the capped 5' end, and the polyadenylated 3' end (12)) into precursor miRNAs (pre-miRNAs; approximately 70-90 nucleotide hairpin structure (13)) in nucleus. The pre-miRNAs are transported to the cytoplasm and further processed by Dicer, into short double-stranded molecules, mature miRNAs (14). If any miRNA machinery component is dysregulated, miRNA maturation is significantly altered, severely affecting the cells' gene expression pattern. The altered expression of important individual miRNA machinery component has recently been suggested to play a role in various human diseases, including SSNHL (15), syncytial virus disease (16), neurological diseases (17), HIV-related lipodystrophy (18), and cancer (1920).
Previously, we evaluated the mRNA expression levels of important miRNA machinery components such as the DiGeorge syndrome critical region gene 8 (DGCR8) and Argonaute 2 (AGO2), and the clinical implication in patients with SSNHL. In the present study, therefore, we investigated the altered regulations of other miRNA-related components such as Dicer and Drosha, and their clinical associations in patients with SSNHL.
MATERIALS AND METHODS
Patients
Altogether, fifty-seven patients diagnosed with SSNHL at Department of Otorhinolaryngology, Dongsan Medical Center between November 2011 and July 2012, were included in the study. Patients were included according to the following criteria: the presence of hearing loss when peripheral blood was collected, unilateral SSNHL of unknown origin, with or without tinnitus and/or vertigo, and no involvement of cranial nerves other than the eighth cranial nerve. SSHNL patients were classified into several clinical characteristics (Table 1). Patients were excluded when having known causes of hearing loss (noise induced, drug induced, Ménière's disease, otitis media, herpes zoster oticus) and familial deafness. Workup included pure-tome audiometry, tympanometry, stapedial reflexes, auditory brainstem-evoked responses, and brain magnetic resonance imaging (in order to rule out acoustic neuroma). Fifty unrelated healthy volunteers, who underwent physical examinations and had the same geographic and ethnic origin as the patient group, were randomly collected as controls.
Specimens and preparation
Peripheral blood was obtained from healthy volunteers and patients with SSNHL. Blood specimens were collected into EDTA tubes to avoid clot. For leukocyte enrichment, an optimized hypotonic lysis procedure with ACK lysing buffer (Gibco, Grand Island, NY, USA) was applied. The tubes were centrifuged and then Phosphate buffered saline (PBS) was added to wash. Finally, only leukocyte enriched-blood cells were collected.
RNA isolation and quantitative real-time RT-PCR
The mRNA expression of components of the miRNA biogenesis including Dicer and Drosha was detected by means of quantitative reverse transcription polymerase chain reaction (RT-PCR). Total cellular RNA was extracted from blood cells using TRIzol (Molecular Research Center, Inc., Cincinnati, OH, USA) and treated with a DNAse to remove DNA. Each cDNA was synthesized form 2 µg of total RNA using M-MLV reverse transcriptase (Promega, Madison, WI, USA). By using the specific primer pairs described in Table 2 and SYBR GREEN Premix (TOYOBO, Japan). Quantitative real-time PCR was performed on the LightCycler® 480 real-time PCR system (Roche Diagnostics, Mannheim, Germany).
Statistical analysis
Prior to statistical analysis, raw qPCR data of Dicer and Drosha mRNA levels were normalized to mRNA level of β-actin. β-Actin was used as a housekeeping gene, and a no template sample was used as a negative control. Then, relative gene expression was calculated by using the comparative CT (ΔCt) method (ΔCt=specific target gene Ct-β-actin Ct) (21). Statistical analysis was performed with SPSS 18.0 (SPSS Inc., Chicago, IL, USA). To compare the mRNA expression levels of miRNA biogenesis-related components between patient groups and healthy volunteers, the data were analyzed using the Mann-Whitney U-test of variance for continuous variables. Correlations between mRNA expressions of interindividual miRNA biogenesis-related components were analyzed by the Pearson's correlation coefficient analysis. The mean value was used as the cut-off value in the present study. Statistical analyses between each miRNA biogenesis-related component and each clinical characteristic were performed by using the Kruskal-Wallis test for categorical variables and the Pearson's correlation coefficient analysis. Generally, a P value of less than 0.05 was established to denote significance in all statistical analyses performed in the study.
Ethics statement
The study protocol was approved by the institutional review board of Keimyung University Dongsan Medical Center IRB (approval # 12-119). All samples derived from the patients with SSNHLs and healthy volunteers were obtained with informed consent under institutional review board-approved protocols.
RESULTS
Expression levels of Dicer and Drosha and mutual relation in patients with SSNHL and healthy volunteers.
To investigate the mRNA expression levels of major RNase components, Dicer and Drosha in the specimens of patients with SSNHL, we determined the expression levels of the selected two miRNA biogenesis-related components in the whole blood cells of patients with SSNHL and healthy controls. Our study revealed that Dicer mRNA expression levels in the specimens of patients with SSNHL were significantly lower than the controls' specimens (P<0.001; Fig. 1). However, in the expression levels of Drosha, there were no significant differences between patients with SSNHL and the controls (P=0.788; Fig. 1). To investigate the significant correlation between mRNA expression levels of Dicer and Drosha in with SSNHL and healthy volunteers, we evaluated the correlations of the two selected mRNA machinery components. As shown in Fig. 2A, there was a significant association between Dicer and Drosha with a Pearson correlation coefficient value of 0.149 in only patients with SSNHL (P=0.004; Fig. 2A), but not in healthy controls (Fig. 2B).
Relationship between mRNA expression levels of miRNA machinery components and the clinical parameters in patients with SSNHL.
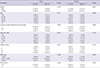
To elucidate the influence of the clinical characteristics on the mRNA expression levels of Dicer and Drosha, patients were grouped according to each clinical characteristic. The clinical characteristics of all 57 patients (mean age 54.43±14.67 yr) with SSNHL were presented in Table 1. As shown in Table 1, there were no significant association between expression levels of specific miRNA machinery components and each clinical characteristic including age, sex, duration of initial treatment from onset (days), Initial PTA, Siegel's criteria, WBC, and ESR.
DISCUSSION
miRNA plays an important role in a wide variety of biological processes in humans including development of human embryonic stem cells (22), cancer (13), infectious disease (23), and heart development and function (24). The miRNA regulation is regulated by miRNA machinery components such as Dicer and Drosha. Dicer and Drosha are enzymes of the RNAse III endoribonuclease family, which are crucial for RNA interference in eukaryotes. Drosha is a component of a multiprotein complex, the microprocessor, which cleaves pri-miRNAs into approximately 60-70 nt hairpin pre-miRNAs in nucleus (25). Dicer is a component of the protein machinery (the RNA induced Silencing Complex [RISC]) which is catalyzing the formation of mature miRNAs from their precursors in the process of miRNA biogenesis (26). Accumulating evidences revealed that dysregulations of the miRNA machinery components Dicer or Drosha are involved in various diseases in humans. For example, mRNA expression levels of Dicer and Drosha were down-regulated in ovarian cancer (19) and endometrial cancer (27). In addition, Dicer expression reduced in the cord blood of infants admitted with severe respiratory syncytial virus disease (16). Although the regulation of miRNA machinery components, DGCR8 and AGO2 has been evaluated in SSNHL, mRNA expression levels of Dicer and Drosha were not elucidated. Therefore, in this study, we wanted to investigate the mRNA expression levels of Dicer and Drosha by RT-qPCR method and their clinical significances in patients with SSNHL and healthy controls.
In the present study, we investigated the expressions and clinical relevance of the two miRNA machinery components in SSNHL. Our data show that Dicer is significantly down-regulated in patients with SSNHL in comparison to healthy controls (Fig. 1). The up-regulated expression of two important RISC components, Dicer and AGO2, has recently been investigated in skin squamous cell carcinoma (2028). In that study, it was as expected because Dicer and AGO2 are both part of the RISC and overexpression of only one RISC component would have been unlikely. On the other hand, a recent study suggested that Dicer and AGO2 are differentially expressed between estrogen receptor negative and estrogen receptor-positive breast cancer (29). We reported that the mRNA expression level of AGO2 is up-regulated in patients with SSNHL (15). Because subjects of each experiment were partially matched, we could not make a comparison of each result. However, we found that Dicer was down-regulated and AGO2 was up-regulated in patients with SSNHLs, suggesting the aspects of gene regulation were similar to our results. Therefore, more study is needed on the regulations of the two components and relationship between each other in many other diseases.
Recently, mRNA expression levels of DGCR8 and AGO2 have been revealed to be positively correlated to each other in patients with SSNHL and controls, suggesting that Dicer and Drosha genes share, at least partly, common mechanisms that contribute to the deregulation of their expression in triple-negative breast cancer (30). So, in this study, the correlation between expression levels of interindividual miRNA biogenesis-related components was evaluated by using the Pearson's correlation coefficient analysis. In only SSNHL patients, a significant correlation between Dicer and Drosha was found (Fig. 2A). Based on the finding that there are significant correlations between Dicer and Drosha, obtained from statistical analyses between SSNHL patients and controls, it is possible to suppose that the changes of correlations from healthy volunteers to patients with SSNHL could be regarded as an epiphenomenon or a pathogenesis of SSNHL.
Although it is not easy to evaluate whether the dysregulated miRNA machinery components are a cause or outcome in the pathogenesis of the diseases, it has been revealed that there were significant correlations between the dysregulated components and clinical parameters (31). Recently, it has been reported that the RNA-induced silencing complex (RISC) component argonaute-2 (AGO-2) is significantly associated with WBC count in SSNHL patients (15). Because Dicer and Drosha are two main enzymes required for post-transcriptional miRNA processing, we therefore investigated whether the mRNA expression levels of Dicer and Drosha are associated with any clinical parameters of SSNHL patients. There are many important factors, which are significantly associated with clinical characteristics of SSNHL. Several known factors are initial hearing loss level, Pure Tone Average (PTA) pattern, age, presence or absence of vertigo and tinnitus, duration of initial treatment from onset, and underlying disease (32333435). Reported evidence revealed that good prognosis in the hearing recovery of SSNHL was associated with absence of vertigo, early treatment (the first 7 days), and initial hearing loss less than 50dB (36). As shown in Table 1, the results indicated that there was no association between altered expression levels of the two enzyme and clinical characteristics, including age, sex, duration of initial treatment from onset (days), initial PTA, Siegel's criteria, WBC, and ESR. Although, mRNA expression levels of Dicer and Drosha were not associated with clinical parameters, as shown in Fig. 1, the cytosolic endonuclease, Dicer is significantly down-regulated in patients with SSNHL. Therefore, the down-regulated Dicer could be correlated with an epiphenomenon or a pathogenesis of SSNHL. Considering the positive correlation between Dicer and Drosha in SSNHL patients, further study on relationship between these miRNA components is needed in SSNHL patients.
In conclusion, we examined the mRNA expression levels of the two critical miRNA machinery components, Dicer and Drosha, and their clinical signification in SSNHL patients' whole blood cells for the first time. Our data demonstrated that Dicer is significantly down-regulated in SSNHL, suggesting that reduced expression of Dicer may play an important role during the development of SSNHL. Considering the deep correlation between Dicer and Drosha in SSNHL patients, further study on relationship between these miRNA components is needed.


 XML Download
XML Download