

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign prostatic hyperplasia (BPH) is a major cause of lower urinary tract symptoms (LUTS) in aging men (1). It is hypothesized that the LUTS observed in men with symptomatic BPH are caused by a combination of increased sympathetic tone in the bladder neck and prostatic urethra (dynamic component) (2), and the increasing size of the prostatic adenoma (static component) (3). BPH is a progressive disease, and prostatic enlargement is associated with a risk of clinical events, including acute urinary retention, and the need for BPH-related surgery (456). In particular, while an increase in prostatic volume (PV) in aging men contributes to BPH/LUTS, it is not only a cause of LUTS, but results in highly variable symptoms among individuals (78). From community-based studies (91011) and data from the placebo arm of several clinical trials (456), the natural history of BPH and risk factors for BPH progression, have previously been evaluated.
Studies have shown that PV and PV change rate is associated with several clinical parameters, including age (810121314), serum prostate-specific antigen (PSA) level (569), and body mass index (BMI) (14151617). Meanwhile, increasing evidence has suggested that PV, and the prevalence of BPH/LUTS, may differ among ethnic groups (11181920). As such, several studies have shown that the PV of Asian men is lower than that in Caucasian men (20212223). However, because most of these studies (212223) were based on populations with BPH/LUTS, there are few data on reference ranges for PV and annual PV change rates in Asian men without BPH/LUTS. In the present study, we analyzed nationwide screening population data to determine normal reference ranges for PV and annual PV change rates in Korean men.
MATERIALS AND METHODS
This was a multicenter, retrospective observational study. Thirteen South Korean University Hospitals from 8 districts (Seoul, Daejeon, Cheongju, Daegu, Yangsan, Busan, Hwasun, and Kwangju) of 6 provinces were selected. Data were acquired as a part of the BPH awareness campaign (Blue Apple Campaign) by the Korean Urological Association. Data were collected from men who underwent a routine health check-up at health promotion centers of the participating hospitals between January 2004 and December 2012.
Men included in the study were aged≥40 yr and had undergone 2 or more serial transrectal ultrasonographies (TRUSs) with a minimum 3-month interval during the study period. To calculate annual PV change rate, only subjects with data from 2 or more TRUSs were included in this study. PV was automatically calculated by elliptical volume measurement (π/6× transverse diameter×anteroposterior diameter×cephalocaudal diameter) (24). Men with initial PV>100 mL; serum PSA level>10 ng/mL; and a history of prostate cancer or BPH-related surgery were excluded. In addition, men with a PV reduction>20% compared with initial PV were excluded because of the high possibility of measurement error or 5-alpha-reductase inhibitor (5ARI) treatment during follow-up (425). After exclusion, 2,967 men who had undergone 2 or more serial TRUSs with a median time interval of 15.9 months (interquartile range [IQR], 12.0-25.9 months) formed the study cohort. Among them, 426 (14.4%) and 106 (3.6%) subjects had undergone 3 TRUSs and≥4 serial TRUSs, respectively. Transitional zone volume (TZV) data were available in 2,392 subjects (80.6%).
All medical records, including clinical, laboratory and TRUS findings, were reviewed. Serum PSA level, self-reported information on co-morbidities, and anthropometric measurements, including height and weight, were collected. Primary outcomes were predicted PV and TZV; secondary outcomes were annual PV and TZV change rates. Subjects were categorized by age into the following groups: 40-49 yr; 50-59 yr; 60-69 yr; and≥70 yr. Subjects were classified by BMI according to the 2000 World Health Organization Asian Pacific Guideline (<23.0 kg/m2; 23.0-24.9 kg/m2;≥25 kg/m2) (26). Subjects were classified by serum PSA level into 4 groups:<1.0 ng/mL; 1.0-1.9 ng/mL; 2.0-2.9 ng/mL; and≥3.0 ng/mL.
For statistical analyses, descriptive statistics were used to examine the demographics and PV distribution of the study cohort. Linear regression analysis was used to determine the predicted mean PV and TZV according to age, BMI, and serum PSA level. Linear mixed effects regression analysis was used to estimate longitudinal change in PV (1027). This estimated average longitudinal change per group (fixed effects), while taking into account individual longitudinal change deviating from the group average curve (random effects). Mean values are reported with their standard deviation (SD) and median values are reported with their 25th and 75th percentiles (IQRs). All tests were two-tailed, with P<0.05 considered significant. Statistical analysis was performed using Stata/SE software, version 12.1 (Stata Corporation, College Station, TX, USA).
RESULTS
The mean age, BMI, serum PSA level, PV and TZV (median with IQRs) for the entire study population was 54.8 (53.0, 48-61) yr, 24.5 (24.4, 22.7-26.2) kg/m2, 1.5 (1.0, 0.7-1.7) ng/mL, 26.7 (24.4, 20.0-30.6) mL, and 11.2 (9.0, 6.0-13.0) mL, respectively. PV according to age, BMI, and serum PSA level is shown in Table 1. PV generally increased with increasing age, BMI, and serum PSA level; the corresponding SD also increased, suggesting high inter-individual variation. The distribution of TZV according to age, BMI, and serum PSA level showed a similar pattern to that of PV.
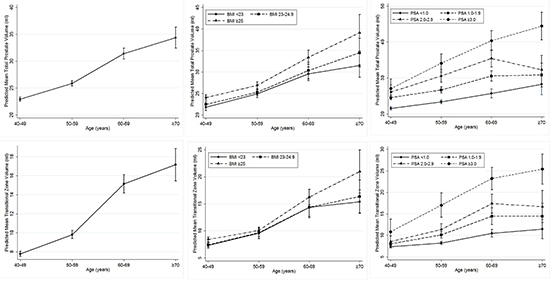
On multivariate linear regression analysis, age, BMI, and serum PSA level were significant predictive factors for both PV and TZV (Table 2, all P<0.001). After adjusting for these 3 variables, a predicted PV and TZV table, with 95% confidence intervals (CIs), was generated (Table 3). For example, using the table, the mean PV and TMZ for a 62-yr-old man with a BMI of 24.2 kg/m2 and a serum PSA level of 2.5 ng/mL could be predicted as 34 mL (95% CI, 30.5-37.5 mL) and 15.2 mL (95% CI, 12.7-17.7 mL), respectively. Fig. 1 shows the predicted mean PV and TZV with 95% CIs, according to age group, and further stratified according to BMI and serum PSA level. This shows that PV and TZV increased significantly with increasing age, BMI, and serum PSA level.
Annual PV and TZV change rates were 0.51 mL/year (95% CI, 0.47-0.55) and 0.32 mL/year (95% CI, 0.29-0.35), respectively. Annual predicted PV and TZV change rates according to age, BMI, serum PSA level, and baseline PV, after considering variation over time, are shown in Table 4. Annual PV change rate according to age was 0.68 mL/year, 0.84 mL/year, 1.09 mL/year, and 0.50 mL/year for men in their 40s, 50s, 60s, and≥70 yr, respectively. Prostate growth rate progressively increased with increasing age until 70 yr, with the most rapid increase between the age of 60 yr and 70 yr. Subjects aged≥70 yr had a reduced growth rate compared with those aged<70 yr.
The annual PV change rate of subjects with a BMI≥25 kg/m2 was greater than that of subjects with a BMI<25 kg/m2. Similarly, there was a tendency for greater PV change rates in subjects with higher serum PSA levels and higher baseline PV. While the 95% CIs according to BMI group were relatively constant, the corresponding 95% CIs increased with increasing age, serum PSA level, and baseline PV; this indicates high inter-individual variation in the subgroups. The general trend in annual TZV change rate for each group (age, BMI, serum PSA level, and baseline PV) were similar to the annual PV change rate.
DISCUSSION
This is the first study to investigate the normal reference ranges for PV and annual PV change rate in Korean men using a nationwide screening population. Our study included data from nearly 3,000 subjects who had undergone 2 or more serial TRUSs to allow analysis of longitudinal PV change and to minimize possible bias due to measurement error associated with a single PV measurement.
Age-specific PV in our study population was slightly higher than that reported in Japanese studies (2022), but lower than that reported in studies of Caucasians (1019), African Americans (1928), or the Dutch (13) (Table 5). Differences in study designs, which range from unselected community samples to clinical cohorts with BPH/LUTS, limit comparisons of our data with those of other studies. The present study reveals that the age-specific PV of a Korean screening population is lower than that of Western community-dwelling men (101328). Similar findings were reported by other clinical studies of Korean (21), Japanese (22), and Taiwanese (23) men.
We found that age, BMI, and serum PSA level were significant predictors of PV and TZV. Therefore, we developed a table for predicting PV and TZV using the 3 variables (Table 2). We believe that our table should be more accurate than simple PV prediction based on a single parameter (age, BMI, or serum PSA level) because the 3 major determinants of PV are adjusted together. Although PV is a determinant of BPH/LUTS, and a risk factor for BPH progression (45678), TRUS-based PV measurement is not feasible in all patients because of lack of availability, inconvenience, and the cost of the examination, particularly in the primary care setting. In this context, our PV table is a useful assessment tool to predict PV in Korean men, using easily obtainable parameters such as age, BMI, and serum PSA level.
Prediction of PV and TZV change rates is another important clinical issue. In our screening population, the estimated annual PV and TZV change rates were 0.51 mL/year and 0.32 mL/year, respectively. Other longitudinal follow-up studies of community-dwelling men report mean annual PV change rates ranging from 0.3 mL/year to 0.6 mL/year (91013). Meanwhile, studies of clinically diagnosed BPH/LUTS patients have reported annual PV change rates of 1.4-2.4 mL/year (629), which is significantly higher than those reported by community-based studies. Of note, the annual PV change rate in our study was comparable to rates reported by community-based studies, which indicates that our study population may represent community-dwelling men. Similar to PV, prior community-based studies have shown ethnic differences in PV change rate (9101320). For example, in an analysis of cross-sectional data, Masumori et al. (20) reported that Japanese men had a lower estimated annual PV change rate than American men (0.3 mL/year vs. 0.6 mL/year). Taken together, Korean men seem to have annual PV change rate that ranges between that of Japanese men and Caucasian men.
We observed that the annual PV and TZV change rates differed depending on age, BMI, serum PSA level, and baseline PV (Table 3). Similarly, prior studies reported that PV change rates differed depending on age (132029), BMI (1617), serum PSA level (69), and baseline PV (1013). Interestingly, annual PV growth rate progressively increased until the age of 70 yr, after which it declined. Although the reason for this finding is unclear, several studies have shown that PV is stable or decreases with age in some men, compared with the general pattern of PV growth (8930). For example, Vesely et al. (8) reported that an increase in PV with advancing age is not continuous, and that PV decreases in those aged 75-79 yr. These findings suggest that a decrease in PV in a proportion of subjects in the older age group may be responsible for the reduced annual prostate growth rate in our subjects aged≥70 yr. Consistent with findings from other studies, we found a tendency for a higher PV growth rate in subjects with a higher BMI, serum PSA level, and baseline PV (691617).
Our study has several limitations. Besides its retrospective nature, the time interval between TRUSs differed among individuals, and the annual PV growth rate was calculated over a relatively short follow-up period (IQR 12.0-25.9 months). Because our PV and TZV estimation was based on TRUS at multiple institutes, inter-observer variation should be considered. In addition, because data regarding 5ARI medication use during the follow-up period were not available, 5ARI medication use in some subjects could have been biased results. Countering these limitations, our PV data were based on a large nationwide population, and were analyzed with appropriate statistical methods. In addition, our PV change rates were based on longitudinal follow-up data in the same men, and are thus more accurate than those derived from cross-sectional data. Subjects in our study were healthy men who underwent a routine health check-up, and most had a PV<30 mL (72.6%) or<40 mL (90.9%). Given that this is a common indication for 5ARI treatment (2129), the proportion of subjects starting 5ARI medication might be expected to be minimal. Given that our data are not restricted to a specific geographical area, but represented a nationwide screening population, we believe that our results are generalizable to the entire adult male Korean population.
We established age, BMI, and serum PSA level-specific reference ranges and annual change rates for PV and TZV in Korean adult men comprising a nationwide screening population. Our results show that age-specific reference ranges for PV in Korean men are lower than those for Caucasian men. Our newly established reference ranges for PV and annual PV change rates in Korean men can be used as a valuable clinical tool for counseling patients with BPH.



 XML Download
XML Download