

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Extragonadal germ cell tumors (EGCTs) comprise 2.3%-8.2% of germ cell tumors (GCTs) (12). EGCTs usually occur in the midline of the body, including the mediastinum, retroperitoneum, and pineal gland. Over 90% of EGCT occurs in young males between the ages of 20 and 35 yr (3). The anterior mediastinum is the most common primary site, which accounts for 50%-70% of all EGCT (2). Patients with a primary mediastinal GCT are usually asymptomatic, or present with cardiopulmonary symptoms due to the compressive effect of a large mass (4). Primary mediastinal GCTs are separated into seminomas and non-seminomatous GCTs. In the mediastinum, teratomas (40%-60%) are the most common GCT followed by mixed GCTs (13%-25%) and seminomas (15%-20%) (56).
Needle biopsy is performed for mediastinal masses prior to chemotherapy, as a diagnostic clue for GCT or to exclude other diagnoses such as a seminoma, lymphoma or another thymic malignancy. Diagnostic elements can be detected on needle biopsy, but non-diagnostic components such as totally necrotic tissue or fibrovascular tissue is also obtained, in the patient who is clinically suspected of mixed GCT. However, when a patient with an anterior mediastinal mass presents with elevation of serum beta-human chorionic gonadotrophin (bHCG) and/or alpha-fetoprotein (AFP), the diagnosis of a mixed GCT could be rendered and subsequent platinum-based chemotherapy is started.
During chemotherapy, GCTs other than teratomas soon regress and decrease in size. Subsequent surgical resection follows in cases with a residual mass or a chemoresistant component. In most cases, the residual histology of the tumor after chemotherapy is comprised of a mature and/or immature teratoma. Since the first-line treatment for a mixed GCT is platinum-based chemotherapy, a detailed histologic component of the pre-existing mixed GCT prior to chemotherapy has not been thoroughly investigated. We aimed to evaluate the histologic components of primary mediastinal mixed GCTs by retrospectively reviewing cases of patients with mediastinal mixed GCTs. Clinical features and histology of the pre-treatment biopsy and post-treatment surgical resection were reviewed.
MATERIALS AND METHODS
Study subjects
Retrospectively, 221 patients were diagnosed with a primary mediastinal GCT at Samsung Medical Center from March 1994 to August 2014 (a 21-yr period). Fourteen patients received subsequent surgical resection after chemotherapy, and among them, 8 patients were clinically and pathologically diagnosed with a mixed GCT and finally included for further evaluation. Clinicopathologic variables including gender, age, level of serum AFP and bHCG, radiologic finding, and overall survival were collected. Slides of the initial needle biopsy before chemotherapy, and those of the surgically resected specimens after chemotherapy were reviewed by two pathologists. Available gross photos of resected specimens after chemotherapy were analyzed with Image J program to assess the proportion of vasculoconnective tissue.
RESULTS
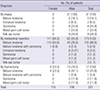
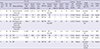
Among the 221 patients, pathologic diagnoses of the primary mediastinal GCT were recorded as a mature teratoma in 172 (77.5%), seminoma in 12 (5.4%), yolk sac tumor in 12 (5.4%), mixed GCT in 11 (6.3%), immature teratoma in 8 (3.6%), and mature teratoma associated with somatic carcinoma in 6 (2.7%) patients. All of the female patients underwent surgical resection, and most of them were diagnosed with a mature teratoma, except for one patient who had a mature teratoma associated with somatic carcinoma. Meanwhile, the male patients had variable types of GCTs, though a mature teratoma was the most common diagnosis. The distribution of diagnoses according to specimen type and histological type is summarized in Table 1.
Fourteen patients received subsequent surgical resection for the mediastinal GCT after chemotherapy. And 8 of these 14 patients were diagnosed with a mixed GCT based on clinical and pathologic information and selected for further evaluation, as shown in Table 2.
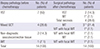
In these 8 patients, pathologic diagnoses on biopsy before chemotherapy were recorded as 1 yolk sac tumor, 4 mixed GCTs, 2 non-diagnostic biopsies containing vasculoconnective tissue and 1 immature teratoma. The specimens surgically resected after chemotherapy were determined to be mostly mature teratomas (5/8, 62.5%) and mature teratomas with a focal immature teratoma (3/8, 37.5%). All 8 patients were male, with a mean age of 23.9 yr (range 13-45 yr), and the average follow-up period was 25.7 months (range 4.7-70.1 months). The mean serum AFP was 1,740.9 ng/mL (range 326.2-5,760.0 ng/mL). Six patients demonstrated an elevated serum bHCG along with AFP, ranging from 25-2,471.2 mIU/mL with an average of 619.4 mIU/mL. After chemotherapy, serum AFP and bHCG were normalized in all patients. Seven of 8 patients experienced an increase and/or no change in tumor sizes. Three patients died of the disease, overall survival was 7 months on average (range 6.5-7.6 months), and 5 patients are alive and well so far, for an average of 36.9 months (ranged 4.7-70.1 months). Two patients were diagnosed with non-diagnostic vasculoconnective tissue on the initial biopsy. Since both patients had elevated serum AFP (2,353.8 ng/mL and 930 ng/mL), and bHCG (2,471.2 mIU/mL and 123.5 mIU/mL), under a clinical diagnosis of mixed GCT, they received 4 and 2 cycles of chemotherapy, respectively. The clinicopathologic profiles of these patients are summarized in Table 3.
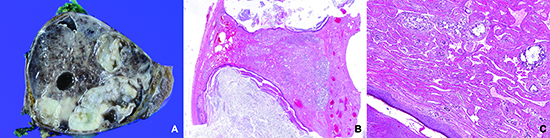
Grossly, all patients exhibited large, well-circumscribed masses with multifocal hemorrhages and cystic changes in the cut surface (Fig. 1). On microscopic examination, all 8 patients had obvious residual teratomatous components. Variable amounts of vasculoconnective tissue were observed in 5 patients (Fig. 2). The vasculoconnective components were intermingled with the teratomatous components, rather than marginated. When the pre-chemotherapy needle biopsies of 5 patients were reviewed retrospectively, a vasculoconnective component was observed in 4 of the 5 patients who had a vasculoconnective component in the resected specimen (Fig. 3A, E, G, and I). In 2 of the 5 resected specimens, moderate to severe cytologic atypia in the vasculoconnective component was found (Fig. 3D, H). In available gross photos of 4 patients, vasculoconnective tissue intermingled with mature teratoma accounted for average 66.3% (range 57.6%-71.5%) of largest cut surface of the resected mediastinal mass.
DISCUSSION
In the current study, we retrospectively reviewed paired needle biopsies and surgical resection specimens of primary mediastinal GCTs before and after chemotherapy in 8 patients. Interestingly, 5 of 8 patients showed predominant vasculoconnective components intermingled with mature teratoma in the resected specimens.
Interestingly, two cases in the present study showed frank cellular atypia in the vasculoconnective component, but it is different from previously described sarcomatous elements of GCTs. According to Malagon et al. (7), sarcomatous component within a GCT is characterized by expansile growth and infiltration into the peripheral surrounding tissue, and morphological and immunohistochemical features should demonstrate an obvious distinct type of sarcoma. In our two cases, an identifiable marginated area or infiltrative features were absent. Furthermore, cellular atypia was not correlated with patient prognosis in the current study, in contrast to the poor prognosis of patients with a sarcomatous component in the study of Malagon et al. (7).
Although there has not been focused research on the vasculoconnective component of mediastinal GCTs, several reports of mature and/or immature teratomas accompanied by hemangiomatous elements have been reported in ovarian GCTs (8910). Since malignancies with neural components, such as glioblastomas and immature teratomas, have been association with vascular proliferation (11), it has been suggested that the neural component of mature teratomas induces vascular proliferation (10). However, in the current study, a neural component was not observed in the 5 resected specimens containing a vasculoconnective component. Ironically, 3 of the 8 resected specimens without a vasculoconnective component had mature glial tissue in mature teratoma. This discordance could be due to the gender inequality between ovarian GCT and mediastinal GCT, and also may be resulted from limitation of the sample size of the current study.
Clinically, 8 patients in the current study had features of growing teratoma syndrome (GTS), which is characterized by the following features: tumor size might be not changed or may even increase during or after chemotherapy, though serum tumor markers are normalized, and surgically resected tumor exclusively shows a mature teratomatous component (12). In such cases, surgical resection rather than chemotherapy is the treatment of choice, to avoid the cardiopulmonary deterioration of patients (1314). In a prior study of primary mediastinal GTS, all patients were young males, had variable prognosis, and demonstrated elevated serum AFP (131516171819202122). In a study by Kesler et al. (21), 5 out of 188 primary mediastinal NSGCT patients had primary mediastinal GTS. Two of 5 patients had foci of angiosarcoma within mature teratoma. However, the angiosarcoma components have not been described clearly, and it is unclear whether it was a true discrete sarcomatous component or more similar to the vasculoconnective component in the present study.
Thus far, only two cases of vascular elements in mediastinal mixed GCTs have been reported (2324). Hui et al. (24) described a mediastinal mixed GCT in a 14-yr-old boy, which was predominantly composed of vasculoconnective elements mimicking a hemangioma and a mature teratoma in the resected specimen after chemotherapy. They concluded that the vasculoconnective tissue might be a result of postchemotherapeutic changes. However, Nuti et al. (23) reported another case of a primary mediastinal mixed GCT in a 37-yr-old male, and over 90% of the tumor was composed of vasculoconnective elements. In that study, the patient underwent surgical resection without prior chemotherapy, because the initial needle biopsy revealed only vasculoconnective tissue, which is suggestive of a hemangioma. Even though there were no comments regarding the patient's serum AFP, it is suspected that the serum AFP would have been elevated, because the resected specimen harbored a yolk sac tumor component together with a large amount of vasculoconnective tissue and a mature teratoma.
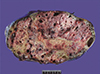
Recently, we encountered a mediastinal mixed GCT in a 19-yr-old male, which is similar to the case of Nuti et al. (23). He was initially diagnosed with a hemangioma from needle biopsy of the anterior mediastinal mass, and underwent surgical resection without further work up or chemotherapy. The resected specimen was composed of a predominantly mature teratoma and hemangioma-like vasculoconnective tissue, with a focal yolk sac tumor, which was consistent with mixed GCT (Fig. 4). The serum AFP level immediately after surgical resection was elevated up to 205.5 ng/mL.
In the current study, we postulated that the vasculoconnective component in previous studies (2324) and the current study would be the intrinsic component of primary mediastinal mixed GCT. These vasculoconnective components are different from sarcomatous components, because they are intermingled with residual teratoma, rather than forming a mass-like lesion or infiltrate into the surrounding tissue. Furthermore, histology of the vasculoconnective component was insufficient for diagnosis of angiosarcoma, though a variable degree of cellular atypia was found in two patients. However, the atypia of the vasculoconnective component seemed to be unrelated to the patient's prognosis and might be on the spectrum of chemotherapy-induced changes, though survival analysis was not feasible due to the small number of patients and short follow-up period of the current study. Together with our recent case described above and previous studies (212324), it is suspected that the vasculoconnective component may exist in mediastinal mixed GCTs as an intrinsic component rather than a postchemotherapy-related change.
When vasculoconnective tissue without a notable GCT component is encountered in the biopsy of a mediastinal mass in a young male patient, it tends to be regarded as a mistargeted specimen, overlooked as a non-diagnostic element, or misdiagnosed as another lesion such as a vascular neoplasm. However, further work up including examination of serum AFP and bHCG levels should be performed to exclude the possibility of an underlying mixed GCT considering vasculoconnective tissue occupies over 50% of mediastinal mass in current study. Also, the risk of development of GTS should be considered when establishing a treatment plan in patients with mediastinal mixed GCTs harboring a vasculoconnective component. Extended prospective studies with larger cohorts are required to further evaluate the clinical implications of the vasculoconnective components of mediastinal mixed GCTs.



 XML Download
XML Download