

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
While sodium is an essential nutrient for humans, a high salt diet is associated with hypertension and cardiovascular disease (CVD) (1, 2, 3, 4). Furthermore, it may be a risk factor of kidney disease, osteoporosis, and even stomach cancer (5, 6). Since these diseases are a major cause of morbidity and mortality in Korea and worldwide, reductions in dietary salt intake could substantially reduce medical costs, and should be a public health priority (7). Recent data on salt intake show that populations around the world are consuming much more salt than is physiologically necessary. In many cases, they are consuming much more salt than the recommendation from the World Health Organization (WHO), which is 5 g salt/day (the equivalent of 2 g sodium/day) (8).
Salt intake can be estimated indirectly from food consumption data or a questionnaire as well as directly by measuring urine sodium. Due to problems with dietary surveys such as the underestimation of sodium intake, assessing 24-hr urinary sodium excretion has become the "gold standard" method of obtaining salt intake data for population surveys (9, 10).
MATERIALS AND METHODS
Study subjects
The baseline survey was conducted from August to December 2013. The study included 104 men and 138 women (total 242; age range, 20-88 yr). The selected subjects comprised a representative sample of Pohang, a city in Korea that has a population of 508,736.
Assessment of salt intake
After obtaining written consent, participants were asked to collect all urine during a 24-hr period starting from the second urine sample on the morning of the collection day and ending with the first urine sample from the following morning. The purpose of salt intake estimation from the collected samples was not mentioned to the participants. Participants were asked to report whether the 24-hr collection was complete or not and to provide information regarding whether the urine collection day was unusual for them. At the survey site, a well-trained health worker measured the total volume. Urine aliquots were stored at -20℃ before being transported to the certified laboratory. The completeness of 24-hr urine collection was assessed by self-reported urine loss and the 24-hr urine creatinine-based method. The 24-hr urine sample was unacceptable if a participant reported urine loss more than one time or if the creatinine index ([24-hr urine creatinine (mg/dL)]/[21×body weight (kg)]) was lower than 0.7 (16).
Urinary sodium and potassium were measured by using an ion-selective electrode method (Modular DPE chemistry; Roche Diagnostics, Germany). Creatinine was measured by using the Jaffe reaction (Kinetic colorimetric assay; Roche Diagnostics, Germany).
All participants were asked to fill out a questionnaire in order to evaluate their dietary salt habits. The questions referred to whether they prefer salty foods, whether they add extra salt before eating, how many times they have Korean soup or stew in one week, how many times they have processed foods, etc. We compared whether the eating habits were correlated with the actual sodium intake.
All analyses were performed by using SPSS statistics, version 20 (SPSS Inc., New York, USA).
RESULTS
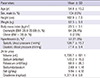
Demographic characteristics are given in Table 1. Among the 242 participants, 104 (43%) were male and the mean age was 54.8±13.2 yr. Mean body mass index (BMI) was 23.5±3.1 kg/m2 and among the men, 64 (26.4%) were overweight (BMI: 25.0-29.99) and 6 (2.5%) were obese (BMI≥30). Fifty-three participants (21.9%) had hypertension, and the mean systolic blood pressure (SBP) and diastolic blood pressure (DBP) were 126.7±15.7 mmHg and 77.4±9.4 mmHg, respectively (hypertension: SBP ≥ 130 mmHg or DBP ≥ 80 mmHg).
The average urine volume was 1,726.7±621.1 mL. Urinary sodium and potassium excretion in the whole group was 170.2±75.9 mM/day and 68.0±28.3 mM/day, respectively. The 24-hr urine sodium to potassium ratio was 2.68±1.16.
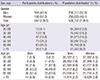
The distribution of the participants and the Pohang city population by age is given in Table 2. There seemed to be more participants over the age of 50 compared with general population distribution even though we selected a representative sample of the Pohang city population, and this sample was statistically significant (P<0.001).
Estimated salt intake in the Pohang city population was 9.9±4.6 g/day. Salt intake in men (10.3±4.7 g/day) was higher than that in women (9.6±4.2 g/day). Overall, 87.6% of the participants (87.5% of the men and 87.7% of the women) had more salt intake than the WHO recommendation (5 g/day).
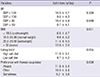
There was no difference in salt intake between high SBP participants and normal SBP participants (10.5±4.7 g/d vs. 9.6±4.3 g/d, P=0.339), but high DBP participants had more salt intake than normal DBP participants (10.4±4.9 g/d vs. 9.7±4.1 g/d, P=0.049) (Table 3).
Salt intake increased as BMI increased (underweight: 6.7±4.7 g/d, normal BMI: 9.6±4.2 g/d, overweight: 11.7±4.5 g/d, obese: 12.8±2.0 g/d, P=0.001) (Fig. 1). Participants who reported that they prefer a high salt diet seemed to have a higher salt intake (11.0±5.1 g/day) than those who do not prefer a high salt diet (9.7±4.2 g/day). This finding demonstrated marginal significance (P=0.055) (Table 3). Furthermore, participants who reported that they frequently consume Korean soup or stew seemed to have a high dietary salt intake (always: 11.8±5.4 g/day, often: 10.0±4.4 g/day, sometimes: 8.2±3.8 g/day, P=0.038) (Fig. 2).
DISCUSSION
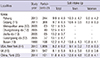
In this study, the estimated daily salt intake through 24-hr urinary collection among adults in Pohang was 9.9±4.6 g/day (sodium 170.2±75.9 mM/day). It is almost 2-times higher than the WHO recommendation. There have been few studies on salt intake by collecting 24-hr urine. In the INTERSALT study (1988) (13), estimated daily salt intake was 12.2±4.2 g among the Busan population in 1988. Furthermore, Jeong et al. (12) reported that daily salt intake in a representative sample of the Korean population (n=215) was 12.7±3.9 g/day. In a more recent study, Kim et al. (11) reported 9.7±0.3 g/day as the mean salt intake of 368 subjects in Goyang city, which is similar to the results of this study. It appears that there has been a reduction in the daily salt intake in the Korean population, but it is still a higher than that in other countries such as the US (8.2±0.2 g/d, 2010, New York) (14) and the UK (8.1±5.8 g/d, 2011, nationwide) (15) (Table 4).
In Korea, salt intake is higher than that in western countries because there is a tradition of adding excessive salt to foods and consuming salty sauces. In previous studies, more than 70% of the sodium intake in Koreans was from Kimchi, Korean soup or stew, and soy sauce (12, 17, 18). In this study, a correlation was demonstrated between participants who enjoy consuming Korean soup or stew and a high salt intake (Fig. 2).
The strong positive correlation between 24-hr sodium excretion and systolic and diastolic blood pressure is well established in many studies (13, 19). However, in this study, only DBP showed a positive correlation with salt intake; perhaps the number of participants was too small.
In the present study significantly higher 24-hr urinary sodium excretion was observed in obese participants in comparison to normal-weight or overweight participants (Fig. 1). The high sodium intake that was observed in conjunction with high urinary excretion in obese subjects has also been described in many other studies (20, 21). However, several mechanisms could explain the association between sodium excretion and an increase in body fat. One explanation could be that a high intake of salt is the result of consuming large amounts of high-energy foods with a high salt content, which could consequently increase the total energy intake. Similarly, studies have shown that a high intake of salt is associated with consuming a large number of soft drinks (22).
Dietary salt intake in Korean adults is still higher than the recommendation of the WHO. Given the health concerns such as hypertension, CVD, obesity, and kidney disease that are associated with excessive salt intake, it would appear that public health initiatives are needed to reduce salt consumption. The aim is to achieve an overall reduction in the Korean population's salt intake by working directly with the food industry to reduce the amount of salt in processed foods. Indeed, campaigns are underway in many countries, such as the US National Salt Reduction Initiative, World Action on Salt and Health (WASH, UK), and the eat low sat campaign (KFDA, Korea). Moreover, a nationwide survey with a 24-hr urine collection is needed to accurately estimate the daily salt intake in Korea.


 XML Download
XML Download