

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the implementation of five, 5-yr economic development plans beginning in the early 1960s, Korea has undergone substantial industrialization. Some consequences of this industrialization has been an increase in the number of workplaces where various hazardous substances are handled, the number of workers employed at these workplaces, and the length of these workers' service periods in these potentially hazardous environments. Accordingly, the number of exposed workers and duration of exposure to hazardous substances has gradually increased over the past several decades, thus increasing workers' risk of developing an occupational disease (OD). Among other examples, such exposure culminated in an outbreak of lead poisoning in workers in a storage battery factory in the 1970s; of mercury, benzene, organic solvent, and chromium poisonings, as well as occupational asthma, in the 1980s; and manganese, carbon disulfide, and ammonia poisonings, in addition to Raynaud's phenomenon, in the 1990s (1).
According to the Korea Workers' Compensation and Welfare Service (KCOMWEL), workers were most frequently compensated for pneumoconiosis (67.1%) and noise-induced hearing loss (16.1%) between 1991 and 2009. However, only 7.2% of the compensated cases reported that their OD resulted from chemical exposure during this period (2), and this percentage decreased from 2009 to 2011 to only 2.0% of all ODs (3). However, outbreaks of ODs resulting from chemical exposures continued to threaten workers' health. For example, in 1981, an outbreak of carbon disulfide poisoning occurred in a rayon yarn factory, and, in 2012, a chemical plant fell victim to a hydrofluoric acid poisoning. However, relevant laws have only recently been amended after extensive review of the available literature. We reviewed the history surrounding the development and establishment of criteria for identifying chemical-induced ODs in the workplace as well as recent amendments to these criteria. Based on these findings, recommendations for further amendments to these criteria are provided.
MATERIALS AND METHODS
Details of the Enforcement Decree of the Industrial Accident Compensation Insurance Act (ED-IACIA) and the Enforcement Decree of the Labor Standard Act (ED-LSA), which are amendments to the criteria for ODs, are described elsewhere in this issue (4).
We thoroughly reviewed domestic and international literature on the history of ODs that resulted from chemical exposures in the workplace. In addition, we reviewed the scope of ODs in the ED-LSA (5) and the specific recognition criteria for ODs in the ED-IACIA (6), since the two acts are closely related. Diseases caused by accidents or pneumoconiosis were excluded from the criteria because special regulations apply. Moreover, the list of ODs published by the International Labor Organization (ILO) (7) was reviewed in detail, and cases of OD in other countries were noted. Newly identified risk factors and ODs were identified using literature on cases reported by the Korea Occupational Safety and Health Agency (KOSHA) and Occupational Lung Diseases Institute of Korea Workers' Compensation and Welfare Service (OLDI of KCOMWEL) to obtain work-related and official domestic exposure statuses of the risk factors and diseases. Last, we considered published literature and the opinions of health professionals who work in occupational medicine. After collecting this information, we found that the guidelines surrounding domestic exposures required revision. Specifically, revisions to the scope, criteria, and systematization of ODs in Korea were specified.
RESULTS
History and laws surrounding chemical-induced occupational diseases
When the LSA was established in Korea in 1954, the LSA specified the scope of ODs in 38 articles in the body of its Enforcement Decree. Since 1954, the only major changes to its content occurred in 1975, when it was amended, and on March 27, 1997, when a specified scope of ODs were established (8). Although the IACIA was established in 1964, it did not stipulate specific criteria for the recognition of ODs until August 27, 1982 when the Ministry of Labor Established Rule No. 71 was amended which defined six criteria for the recognition of ODs that was developed (9). This rule not only defined criteria for benzene, trichloroethylene, lead, and mercury amalgams exposures but also was the first to stipulate the role of chemical factors in ODs. The recognition criteria were amended several times until the Ministry of Labor Established Rule No. 247 was amended on July 21, 1994, which added criteria for recognizing carbon disulfide, vinyl chloride, tar, manganese, chromium, and cadmium exposure-related diseases (10, 11, 12, 13, 14). On May 1, 1995, the Ministry of Labor amended the Enforcement Rule of the IACIA (ordinance no. 97) with the addition of revised criteria for identifying ODs (15). These criteria were then published in the ED-IACIA as a schedule to the Enforcement Decree on July 1, 2008 (16).
The most important event in Korea's history of ODs caused by chemical exposure was the first documented case of carbon disulfide poisoning in 1981. Although the first case of carbon disulfide poisoning was reported in a German rayon factory in the 1890s, the first case of carbon disulfide poisoning in Korea helped to reveal the problems surrounding chemical-induced diseases. Following a subsequent outbreak in 1990, approximately 1,000 n workers were diagnosed with carbon disulfide poisoning until 2009 (2). In the US, Europe, and Japan, an outbreak of carbon disulfide poisoning occurred in the 1950s throughout numerous viscose rayon factories. As a result, manufacturers moved their factories to other countries. US manufacturers moved their factories to Central and South America, and Japanese manufacturers moved their factories to Korea and Taiwan (17). Following this trend, Korean manufacturers moved the Wonjin Rayon Company to China in 1993 after operating in Korea for 31 yr.
Formal criteria for the recognition of carbon disulfide poisoning were outlined in the Ministry of Labor Established Rule No. 205 on November 1, 1991 (12). After the Ministry of Labor requested that the Korean Society of Occupational and Environmental Medicine establish these criteria, Korea University was the first to present it in 1991 (12). Meanwhile, the Graduate School of Public Health at Seoul National University conducted an epidemiological investigation on 208 retired and 1,164 active workers from August 1991 to March 1992. In May 1992, they reported that 52 workers had been poisoned and 85 were suspected of having been poisoned, according to the available criteria at that time. However, in 1992, the Association of Physicians for Humanism presented different recognition criteria. In February 1993, the Occupational Safety and Health Research Institute (OSHIRI) of the KOSHA held an Occupational Disease Deliberation Committee meeting where committee members and clinical specialists in ophthalmology, neurology, nephrology, and family medicine developed an amendment to the original criteria. This amendment was subsequently included in the Ministry of Labor Established Rule No. 234 in May 1993 (13, 18).
In 1985, the first reported case of inorganic mercury poisoning occurred in a 16-yr-old n female who was working at a thermometer manufacturing factory and developed an organic mental disorder (19). This case was followed by the subsequent death of a 15-yr-old n worker who worked for only 2 months at a precision instrument manufacturer in Seoul on July 2, 1988 (20). These incidents raised concerns about OD as well as the risk of carbon disulfide poisoning among workers at the Wonjin Rayon Company. Fortunately, Criteria for the recognition of mercury poisoning were already included in the Ministry of Labor Established Rule No. 71 (dated Aug 27, 1982) (9).
Lead poisoning was the most common cause of chemical-related OD. In Korea, 7one notable outbreak of lead poisoning occurred among storage battery workers in 1982 (21). However, the diagnostic criterion for lead poisoning was not revised until 2003 by the Ministry of Labor to include a blood lead concentration of 40 µg/100 mL or higher (from 60 &g/100 mL or higher) (9, 16). In addition, the first report of manganese poisoning occurred in 1991 among ore crushing workers (22, 23). After this report, criteria for the recognition of manganese poisoning were added. Furthermore, the Ministry of Labor subsequently added criteria for vinyl chloride, tar, manganese, chromium, and cadmium poisoning based on the results of previous studies.
Recommended reforms to the established criteria
Before its amendment, the ED-LSA contained 38 articles that described 65 hazardous factors, 41 of which are chemical factors, and related symptoms, signs, and diseases (5). However, the ED-IACIA addressed 23 articles before it was amended and described 73 hazardous factors, 40 of which were chemical factors (6). A similarity between the specific criteria for the recognition of ODs and the scope of ODs presented in the ED-IACIA and the ED-LSA is that neither act classified each article by cause or disease. Under the LSA, diseases due to chemical, physical, and biological factors were simply enumerated, but in no particular order. In the IACIA, the specific criteria for recognition of ODs focused on hazardous factors rather than specific diseases, except for cerebro-cardiovascular, musculoskeletal, liver, and occupational skin diseases, and most of the reported diseases were related to chemical exposures. In addition, diseases such as central nervous system disorders resulting from acute poisoning, which have the same conditions but are caused by various factors, were included in the criteria, but the diverse chemicals were not clearly listed.
Therefore, before the LSA was amended, the most pressing issue regarding the description of chemical-related ODs was clarification of the systematic descriptions of each OD by its hazardous factor(s). The published criteria and descriptions for identifying ODs under the IACIA also required revisions so that items were reported separately for each anatomical system. First, the classification system used for hazardous chemicals had to be revised before amending the IACIA. Although the original IACIA comprehensively described chemical poisoning and its symptoms as well as information about organic solvents, other published criteria reported only one risk factor and disease for each hazardous chemical. In addition, the original IACIA provided no guidelines to aid in identifying when a worker had been exposed to a diverse range of chemicals, and the reported guidelines were slightly different from those presented under the ED-LSA. Last, the original IACIA did not address all of the chemicals subject to a medical examination after a worker was exposed. These shortcomings lack consistency, which create difficulties in preventing further exposure and disease. These published criteria also fail to recognize and stipulate chemical dosage, exposure level, latent period, and other factors, which may differ depending on the characteristics of the disease.
To maintain and improve these criteria, newly recognized hazardous chemicals should be added. To this end, we suggest that the criteria for identifying ODs be updated to include ODs that have since been recognized through epidemiological investigation. In addition, hazardous chemicals that have not been linked to diseases in Korea but appear in the list published by the ILO of chemical-related ODs should be added to the n literature. However, we recognize that these revisions would greatly expand the length of the legislative bill, therefore making its application in the workplace difficult for workers, employers, and experts/administrators.
To ensure a concise the legislative bill is drafted, only updated criteria that was not already included in previous legislation should be added to the bill. Furthermore, the chemicals presented in the LSA and the IACIA should be merged to minimize overlap between these documents. To this end, ensuring the maximal inclusion and classification of diseases due to exposure to chemical factors by anatomical system, as well as the description of acute poisoning due to exposure to chemical factors in individual items, is desirable. Therefore, any amendments to the LSA should be organized and listed according to the types of hazardous chemicals, and newly recognized chemicals related to ODs should be listed. In addition, a rational anatomical and systematic classification system should be developed in the IACIA for each specific criterion used to identify ODs.
Status of chemical-Induced occupational diseases in Korea
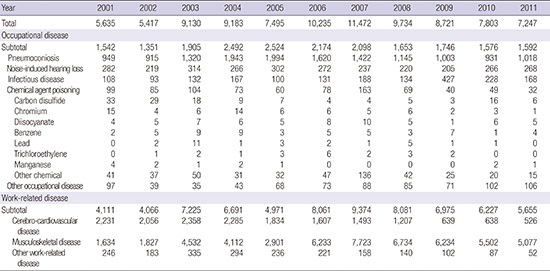
Table 1 shows the number of times a worker was compensated for an OD by year from 2001 to 2011 in Korea (3). Over this period, 4.1% and 0.9% of all ODs and all compensable ODs were chemical-induced ODs, respectively. Recently, both the absolute number of cases and the percentage of chemical-induced ODs have been decreasing. Among all chemical causes of OD, exposure to carbon disulfide was the most frequent at 15.7% (134 cases), followed by chromium at 8.0% (68 cases), diisocyanates at 7.3% (62 cases), benzene at 6.3% (53 cases), lead at 3.2% (27 cases), trichloroethylene at 2.4% (20 cases), and manganese at 1.5% (13 cases).
There are three possible reasons why chemical exposure was found to cause a small percentage of all ODs. First, the risk of being exposed to a concentration high enough to cause acute poisoning may be low. Second, there is a small chance that workers were able to obtain approval to receive medical care services for more than 4 days to treat a chemical poisoning; the incidence of an OD must be approved under the IACIA. Last, it remains difficult to collect evidence of chemical poisonings because there is a lack of general knowledge about exposure to hazardous chemicals in the workplace. These limitations apply to all chemical-induced ODs including those not yet known to be hazardous according to epidemiological investigation.
Indeed, the existence of new ODs are increasingly identified through epidemiological investigation. For example, methyl bromide poisoning was first documented in 2000 in a 20-yr-old man who experienced central nervous system disorders after 2 months of fumigation work (24). This case was followed by 3 cases of methyl bromide intoxication reported before 2001 and an outbreak of methyl bromide intoxication among 6 workers who showed symptoms of central and peripheral nervous system disorders in 2008 (25).
The first reported case of organotin intoxication, which manifested in the central nervous system, was in 2005 in a tank cleaner who had worked for several different companies over the previous 8 yr (26). After several outbreaks of toxic hepatitis after being exposed to dimethylformamide, which is used to produce synthetic fiber and leather, a study was conducted in Korea in 1991 (27). In 1995, a suspicious case of fulminant hepatitis that was attributable to DMF was reported (28) followed by reports of toxic hepatitis in 1999, 2005, and 2006 (29, 30, 31). On September 27, 2012, approximately 8-12 tons of 100% anhydrous hydrogen fluoride were released for approximately 8 hr while a tank transport vehicle was being moved (32). This accident resulted in the death of five workers, posed serious health hazards to residents, and damaged crops and facilities near the industrial complex area (32).
Although the percentage of chemical-induced ODs is smaller than that of other risk factors, maintaining and updating these criteria are important because new chemicals continue to be introduced into the workplace.
Changes to the listed chemicals before and after amendment to the ED-IACIA
Table 2 lists the hazardous chemical agents that were considered to be associated with ODs before and after the ED-IACIA was amended. The amendment resulted in the addition of eight chemicals: organotin, methyl bromide, carbon monoxide, nitrogen dioxide, hydrogen sulfide, hydrogen cyanide, hydrogen fluoride, and phosphorus, resulting in 21 total chemicals. Among the eight new chemicals in the ED-IACIA, organotin and methyl bromide were also recognized for the first time in the amendment of both the IACIA and LSA. However, carbon monoxide, nitrogen dioxide, hydrogen sulfide, hydrogen cyanide, and phosphorus or its compounds were recognized as risk factors for ODs in the ED-LSA before they were added to the ED-IACIA. In both the IACIA and LSA, the terms "fluoride or its compounds" was changed to read "hydrogen fluoride" or "hydrofluoric acid" (5, 6, 33).
Results of the amendments
The section entitled the "Scope of ODs" under the ED-LSA describes the scope of ODs caused by hazardous chemicals. Except for occupational injuries, factors that cause ODs are specified as physical, chemical, or biological factors. Notably, this section includes all chemical-induced cancers under the subheading for occupational cancers, not under diseases due to chemical factors. The IACIA criteria for the recognition of ODs are listed by body organ, except for diseases resulting from acute chemical poisoning. In addition, criteria for the recognition of occupational cancer are presented separately from that of other diseases, which are listed by body organ.
Table 3 lists all chemical-induced diseases and their respective chemical agent(s), which appears in the amended ED-LSA (34). The most important difference between the original and amended criteria is that all diseases are presented in one section of the amended list. Other important changes include corrections to improper disease name expressions; the removal of substances not likely to appear in the workplace or substances whose toxicity is uncertain; and the addition of cadmium, cobalt, and organotin, which were recently recognized as causative agents of ODs using epidemiologic studies. Cadmium and organotin were added because they were included in all versions of the IACIA but not in the LSA, and cobalt was added because of its link to asthma. In addition, criteria for intoxication and incident disease after being exposed to organic solvents such as toluene and xylene were added to be consistent with the IACIA. Pneumoconiosis, cellulitis, skin diseases, metal fume fever, burns, and conjunctivitis have been clearly described in terms of their specific criteria, while all other diseases have been described in terms of their relevant hazardous risk factors. Information about skin diseases resulting from filature or spinning work and poisoning by acetone or other solvents were removed because of their low prevalence.
The criteria for identifying chemical-induced diseases such as acute poisoning, under the IACIA are listed in Table 4 (33). In contrast to the LSA, which presents relevant hazardous factors and the diseases that may result, the IACIA categorizes this information according to the symptoms and signs of disease in detail. One difference from the original criteria is that diseases, symptoms, and signs that may result from repeated exposures to many hazardous factors are presented together with all causative hazardous factors in the revised version. The most representative example of this is the criteria for central nervous system disorders. Only vinyl chloride was presented as a causative substance in the original criteria, but methyl bromide, organotin, and carbon monoxide were added to the revised version. In addition, trichloroethylene was added as a causative substance for symptoms of decreased consciousness after being exposed to organic solvents such as toluene, xylene, and normal hexane.
These criteria have been largely divided into sub criteria for diseases caused by acute poisoning or hazardous chemicals. The symptoms and signs of diseases from acute poisoning (temporary exposure to a large quantity of a chemical) are described separately from the anatomical classification system. Many of the diseases resulting from acute poisoning affect the nervous system because most chemicals are associated with the toxicity of the nervous system. In addition, the criteria has been expanded to include recognition of diverse diseases, symptoms, and signs, such as mucosal irritation, respiratory diseases, skin diseases, and renal diseases following toxic substance decomposition. Overall, the section that describes chemical-induced diseases has not undergone many changes, except for diseases that correspond to a specific organ system (the digestive system excluding the liver, oral cavity, and urogenital system), which was reclassified in this amendment. Except for organic solvents such as toluene and xylene, descriptions of most individual chemical factors have been presented, and the original criteria for carbon disulfide-induced diseases have been presented without any changes.
DISCUSSION
Chemical poisoning, ranging from carbon disulfide to hydrofluoric acid poisoning, continues unabated due to lack of information, knowledge, and awareness of safety guidelines to avoid occupational hazards. Although the scope of OD under the amended ED-LSA is based on classification of OD by factors, the specific criteria for the recognition of OD under the ED-IACIA are based on an anatomical system. Some ODs, such as those of the digestive system except liver, urogenital system, and mouth, are not currently classified by anatomical region under the ED-IACIA. Therefore, all chemical-induced diseases may not fall under the specific criteria for recognition of ODs under the ED-IACIA by anatomical classification. Some diseases may be better classified by their chemical causes such as "diseases due to chemical factors such as acute poisoning," which could describe certain neural, respiratory, and cerebro-cardiovascular diseases. In Korea, many diseases of the digestive and urogenital systems are not considered ODs, and no attempt has been made to include these in the list of ODs. However, more information about diseases of specific systems is necessary in the ED-IACIA to improve the level of clarity and communication among workers, employers, and compensation experts.
Chemical agents in the ILO list of ODs that do not appear in the amended ED-IACIA and ED-LSA include the metals 1) beryllium, 2) vanadium, 3) antimony, 4) thallium, 5) osmium, 6) selenium, 7) copper and 8) platinum; chemical compounds 9) nitroglycerin and other nitric acids and 10) esters, alcohols, glycols, and ketones; the acrylonitrile and gaseous agents 11) ozone and 12) phosgene; and 13) pharmaceutical agents or 14) corneal irritants such as benzoquinone (7). Although the amended ED-LSA made an effort to include a comprehensive list of chemical agents that are "toxic irritants and other hazardous chemicals," future amendments to the ED-LSA should include all chemicals listed by the ILO. Moreover, future amendments to the LSA should include consistent, detailed descriptions of hazardous concentrations and periods of chemical exposure. This information was not included in the recent amendments because of limitations in the scientific evidence, such as a short study period, and temporal limitations in the revision of legislative bills.
As industrialization steadily progresses, particularly in developing countries and underdeveloped countries, the emergence of chemical-induced diseases will steadily and unavoidably occur, in part due to the introduction of new chemicals and lack of knowledge surrounding existing chemicals. However, the health effects of chemical exposure and countermeasures for decreasing or avoiding exposure can greatly assist in protecting workers' safety and health, thus continuous investigation is required.



 XML Download
XML Download