

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The creation of a skin flap is a simple and reproducible method for skin defect reconstruction. However, ischemic necrosis due to insufficient local blood supply is a serious complication of this procedure. Insufficient arterial blood supply and inadequate venous drainage are frequent occurrences and can result in skin flap death, especially in the distal portion where the blood flow is most likely to fail. Various surgical and non-surgical techniques have been devised to increase flap perfusion, thereby reducing the risk of ischemia. Among these, many reports have focused on increasing the local blood supply through inducing angiogenesis by means of growth factors such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), or platelet derived growth factor (PDGF) (1, 2, 3, 4, 5, 6, 7, 8).
Hepatocyte growth factor (HGF) is a pleiotropic growth factor with an apparent molecular weight of 80 kDa that is capable of inducing cellular proliferation, migration, and invasiveness (9). One of the important activities of HGF is to stimulate angiogenesis of various types of cells. HGF is a potent angiogenic factor and can act on endothelial cells directly or indirectly to induce angiogenesis (10, 11, 12). Moreover, HGF stimulates the production of functional vessels in the ischemic zone by promoting the migration of vascular smooth muscle cells as well as endothelial proliferation (13). HGF has been reported to stimulate angiogenesis in rabbit, rat, and mouse ischemic hindlimb models of diabetes and high concentration lipoprotein (14, 15, 16, 17). In addition, HGF has been reported to have more potent angiogenic activity than VEGF and FGF in vitro (2). Because of its potential angiogenic benefits, several studies have investigated whether HGF can increase skin flap perfusion (18). Although skin flap neovascularization can possibly be improved by HGF, its use in a clinical setting is hampered by this protein's short half-life, poor bioavailability, and the consequent need for frequent administration to sustain long-lasting effects. For HGF to be applied clinically, an efficient drug-delivery system or alternative ways to realize the pharmacological effects of this growth factor need to be developed (19).
Recent studies have shown that therapeutic angiogenesis induced by gene therapy can result in a more sustained and efficient therapeutic outcomes. Angiogenic growth factors have been evaluated in this context, and therapeutic angiogenesis using angiogenic growth factor therapy has been reported to have beneficial effects in human patients with critical limb ischemia and myocardial ischemia (2, 12, 20, 21). Of the various gene delivery systems developed for therapeutic angiogenesis, adenoviruses have been widely used because of their ability to transfer relatively large genes. Therapeutic angiogenesis by gene delivery has been used to enhance the survival of skin flaps.
Inadequate perfusion, which is the most common cause of distal flap necrosis, could potentially be avoided by administering HGF to the skin flap. We therefore developed an HGF-expressing adenovirus and introduced this adenovirus into ischemic skin flaps to investigate the ability of subdermal HGF-expressing adenovirus gene therapy to augment blood perfusion and flap survival in a rat skin flap model.
MATERIALS AND METHODS
Animal preparation
The Institutional Animal Care and Use Committee of Yonsei University approved all animal protocols (2011-0143). Thirty male Sprague-Dawley rats weighing 300 to 350 g were used. Rats were maintained in a regulated airflow room in which temperature, humidity, and light were controlled. The rats were divided into three experimental groups. The HGF virus group was pretreated with a replication-incompetent adenovirus expressing HGF. The rhHGF group was pretreated with recombinant HGF (rhHGF). The PBS group was pretreated with phosphate buffered saline (PBS). All three groups were pretreated by a subdermal injection distributed evenly across a total of eight injection points of the flap 2 days before flap elevation and immediately after flap elevation.
Generation of HGF-expressing adenoviruses
An HGF-expressing adenovirus (dE1-RGD/lacZ/HGF) was provided by Dr. Chae-Ok Yun (22) of Department of Bioengineering, College of Engineering, Hanyang University (Fig. 1). To develop an adenovirus encoding the RGD peptide (9-amino acid sequence of CDCRGDCFC) between the HI-loop of the fiber knob, two complementary oligonucleotides encoding RGD (boldface and italicized) were first synthesized and annealed to form a DNA duplex. This DNA duplex was designed to contain a BamHI overhang on the 5' end and an MroI overhang on the 3' end (underlined in the primer sequences below). The oligonucleotide sequences of the primers were 5'-gatccTGTGACTGCCGCGGAGACTGTTTCTGCt-3' and 5'-ccggaACAATGACGGCGCCTCTGACAAAGACGg-3'. The annealed DNA duplex was then digested with NcoI and MfeI and cloned into pSK5543, generating a pSK [5543-RGD] adenovirus fiber shuttle vector. The pSK [5543-RGD] shuttle vector was then linearized by SacI and XmnI digestion, and the lacZ-expressing adenoviral vector pdE1/lacZ was linearized by SpeI digestion for homologous recombination in Escherichia coli BJ5183, resulting in the pdE1-RGD/lacZ adenoviral vector. To construct an adenovirus expressing lacZ and HGF at the E1 and E3 regions, respectively, pdE1-RGD/lacZ was linearized by SpeI digestion and then co-transformed into Escherichia coli BJ5183 with the PvuI-digested pSP72-E3/CMV-HGF shuttle vector for homologous recombination, yielding the pdE1-RGD/lacZ/HGF adenoviral vector. All adenoviruses were developed and multiplied in 293 cells. Viral particle numbers were calculated from measurements of absorbance at 260 nm (A260), where 1 absorbency unit is equivalent to 1012 viral particles/mL.
Experimental protocol
The rats were anesthetized with isoflurane (Aerane®; Ilsung Pharmaceuticals, Seoul, Korea) and by intraperitoneal injection of a zolazepam-tiletamine mixture (30 mg/kg, Zoletil®; Virbac, Carros, France) and Xylazine (10 mg/kg, Rompun®; Bayer, Seoul, Korea). Body hair was removed from the entire dorsal area using depilatory cream. A 3×9 cm flap, including the panniculus carnosus muscle, was created from the dorsum of the prepared rats, and this flap was vertically elevated with its base on the caudal portion. To block new blood supply from the bed, a silicone sheath (Bioplexus Corporation, Saticoy, CA, USA) was placed on the flap bed and the flap was sutured with a 4-0 nylon suture to its original location. To prevent the rats from biting the flaps on others after recovery from anesthesia, each rat was placed in a separate cage. Just before injecting the rats, 1×107 plaque-forming units (PFU) of HGF-expressing adenovirus in a final volume of 800 µL, 500 ng of rhHGF (Abcam Inc, Cambridge, MA, USA) in a final volume of 800 µL, or 800 µL of PBS were loaded into a 1-mL syringe with a 27-gauge needle. Injections were made into the subdermal layer of the entire area of the mapped skin flap (eight injection points) 2 days before flap elevation and immediately after flap elevation.
Evaluation of skin flap survival rate
The elevated flaps were returned to their original position and flap survival was checked on postoperative days 3, 7, and 10. On days 3, 7, and 10, digital photographs were taken of the flap and these images were input into the Scion image program (NIH-Scion Corporation, Frederick, MD, USA). Using this program, the length of the image was converted to the actual length and the surface area was calculated. The survival area was determined by subtracting the demarcated area of necrosis from the total surface area. Flap survival was calculated as the ratio of the viable surface to the total surface area and expressed as a percentage.
In vivo measurement of microcirculation in the skin flap
To assess changes in blood flow in the skin flaps, we used the Periflux® System 5000 (Perimed AB, Jarfalla, Sweden). Serial measurements of skin vascularity were taken from four areas (proximal, mid-proximal, mid-distal, and distal portion) using laser Doppler flowmetry assessment of the initial status before injection of HGF expressing adenovirus, rhHGF, or PBS immediately before flap elevation, immediately after flap elevation, and 3, 7, and 10 days after repositioning of the flap. Data were measured at the four flap points at 1-min intervals and the mean value was obtained. The ratio of blood flow was calculated as the blood flow immediately after flap elevation or that on postoperative day 3, 7, and 10 divided by the initial blood flow before injection.
Immunostaining
Samples (1×1 cm) were taken along the longitudinal midline 5 cm from the base of the skin flap on postoperative day 10 in the three experimental groups and fixed with 10% formaldehyde. Formaldehyde-fixed tissues were transferred into a paraffin-embedded block, mounted on a slide, and stained with hematoxylin and eosin for histological examination.
To detect HGF in tissues, paraffin sections were permeabilized with 0.1% Triton X-100 solution. After washing three times, samples were blocked with 10% normal goat serum for 1 hr at 37℃ and incubated with goat anti-HGF antibody (R&D Systems, Inc.) at 4℃ overnight and then with Alexa fluor 594 (Red)-labeled donkey anti-goat IgG (Invitrogen) at 37℃ for 1 hr. Finally, the samples were incubated with 4,6-diamidino-2-phenylindole (DAPI; Sigma-Aldrich, St. Louis, MO, USA) for counterstaining and then observed using a BX51 fluorescent microscope (Olympus).
Tissue sections were pretreated with a 3% hydrogen peroxide solution for 10 min to block endogenous peroxidase and were then treated with protein block serum-free reagent (DAKO, Carpinteria, CA; X0909) for 30 min to prevent non-specific reactions. Sections were incubated at 4℃ overnight with primary antibodies (rabbit anti-vascular endothelial growth factor (VEGF); RB-222-P; Laboratory Vision, Fremont, CA, antimouse platelet endothelial cell adhesion molecule-1 (PECAM/CD31) polyclonal antibody; M20, Santa Cruz Biotechnology, Santa Cruz, CA, USA) and then incubated at room temperature for 20 min with secondary antibodies from the DAKO Envision Kit (DAKO).
To calculate the amount of neovascularization, CD-31 positive vessels were counted and the number of vessels at each high power field (×200) was recorded. The expression level of VEGF was semi-quantitatively analyzed using MetaMorph® image analysis software (Universal Image Corp). Results are expressed as the mean optical density (OD) of eight different digital images.
Statistic analysis
Statistical analyses were performed using SAS statistical software (version 9.2, Cary, NC, USA). Each measurement is reported as the mean±standard deviation. Differences between groups were assessed by one-way ANOVA adjusted by Bonferroni's correction. P values of <0.05 were considered significant.
RESULTS
Expression of HGF in the skin flaps
To evaluate if injection of HGF-expressing adenoviruses into the skin flap resulted in the expression of HGF in the skin flaps, we analyzed HGF expression by immunofluorescence staining on postoperative day 10 after local injection of HGF-expressing adenovirus (dE1-RGD/lacZ/HGF) or rhHGF. As expected, significantly stronger immunoreactivity for HGF was found in the HGF-virus group than in the rhHGF group (Fig. 2).
Effect of HGF-expressing adenoviruses on skin flap viability
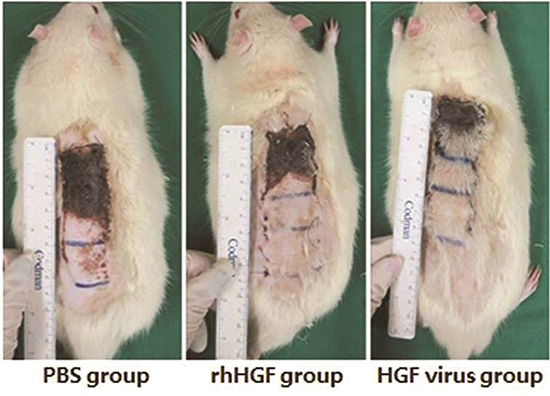
In the PBS group, partial flap necrosis was observed and there was a significant, visible difference in the extent of necrosis among the three groups based on the digital photographs obtained on postoperative day 10 (Fig. 3A). Scion image program analysis on postoperative day 10 revealed that the skin flap survival area was significantly increased in the HGF virus group compared to the rhHGF and PBS groups (71.4%±5.9%, 63.8%±6.4%, and 39.2%±13.0%, respectively) (P=0.025) (Fig. 3B).
The administration of HGF in the form of a recombinant protein or by gene delivery resulted in a higher rate of skin flap survival than PBS injection, and the highest rate of skin flap survival was observed in the adenovirus gene delivery group.
Effect of HGF-expressing adenoviruses on the blood flow in the skin flap
Before flap elevation, the initial blood flow in the flap was not significantly different among the PBS group, rhHGF group, or HGF virus group (22.15±8.95 perfusion units (PU), 24.46±8.63 PU, and 22.97±6.19 PU, respectively). Blood flow as measured by laser Doppler flowmetry increased in both the rhHGF group and HGF virus group after injection, and the increase in blood flow was especially marked in the distal half of the skin flap.
In the mid-distal portion of the skin flap, the blood flow ratio was significantly increased on postoperative days 7 and 10 in the HGF virus group compared with the other two groups (0.56±0.27, 0.71±0.35, respectively, P=0.028) (Fig. 4A). In the distal portion of the skin flap, there was a significant increase in the ratio of the blood flow in the HGF virus group (0.56±0.50, 0.35±0.47, P=0.017) on postoperative days 3 and 7 compared with the other two groups. Blood flow to the skin flap was maintained in the HGF virus group until postoperative day 10 in contrast to the other two groups (Fig. 4B).
Effect of the HGF-expressing adenoviruses on capillary density in the skin flap
To calculate the amount of neovascularization, we performed CD31 immunohistochemical staining. More CD31-positive vessels were observed in the HGF virus group than the other two groups (Fig. 5A-C). A comparative analysis of the number of vessels at different high power fields (×200) revealed no significant difference in the number of CD31-positive vessels between the PBS group (3.8±0.76) and rhHGF group (5.8±0.80). However, the number of CD31-positive vessels was significantly higher in the HGF virus group (8.7±2.91, P=0.037) than the PBS and rhHGF groups (Fig. 5D).
Effect of the HGF-expressing adenoviruses on VEGF expression in the skin flap
Staining for VEGF immunoreactivity was higher in the HGF virus group than the other two groups (Fig. 6A-C). Semi-quantitative analysis using MetaMorph® image analysis software (Universal Image Corp.) showed that VEGF expression was significantly increased in the rhHGF group and HGF virus group (19,411.0±4,916.6 integrated OD and 29,439.4±6,169.1 integrated OD, respectively) compared with the PBS group (9,844.4 ±7,591.0 integrated OD). Furthermore, VEGF expression was significantly higher in the HGF virus group than the rhHGF group (P=0.029) (Fig. 6D).
DISCUSSION
Distal skin ischemic necrosis is a common complication of skin flap surgery. Among the methods that have been devised to increase skin flap perfusion to reduce the risk of skin ischemic necrosis, those methods that increase the local blood supply through growth factor-stimulated angiogenesis induction using growth factors such as VEGF, FGF, and platelet-derived growth factor (PDGF) have reported promising results (1, 2, 3, 4, 5, 6, 7, 8). To induce angiogenesis by means of growth factors, recombinant proteins or genes encoding the growth factor of interest need to be administered to the site of interest. Recombinant protein therapy is the most practical means to administer angiogenic agents. However, a very high dose of protein may be necessary to achieve adequate uptake, which often results in an unacceptably high adverse event rate. Moreover, a single administration of growth factor is unlikely to result in sufficient growth factor levels for a beneficial result to be observed. In contrast, administration of the gene coding for the protein of interest can potentially result in sustained local protein secretion with minimal adverse effects. Furthermore, the efficacy of gene uptake has been shown to be enhanced in ischemic tissue (12). Therefore, we performed gene therapy to improve ischemic skin flap survival.
Of the various gene carriers that have been investigated, adenoviruses are widely used because of their ability to transfer relatively large genes to dividing or non-dividing cells (23, 24). Several experimental studies have reported that administration of VEGF-expressing adenoviruses can result in therapeutic angiogenesis (7, 21, 25). Huang et al. (7) reported a correlation between flap survival and injection of an adenovirus expressing VEGF-165. Recently Zheng et al. (25, 26) reported even greater flap survival due to increased VEGF expression by incorporating the VEGF gene into vectors using genetic transformation of mesenchymal stem cells. Our research group recently reported increase of flap survival with relaxin expressing adenovirus (27).
In this time, we generated an HGF-expressing, replication-incompetent adenovirus (dE1-RGD/lacZ/HGF) and subdermally injected this virus into rat skin flaps. The function of RGD sequence in HGF-expressing adenovirus is to promote gene delivery into cells (27). These replication-incompetent adenoviruses have limited anti-cancer gene therapy effects in that their anti-cancer effects are restricted to adjacent infected cells. However, they are effective at delivering genes to ischemic skin flaps to augment blood flow, as the results of this study show.
HGF is a pleiotropic growth factor with a variety of biological effects. HGF has been shown to function as an angiogenic factor in vitro, and induction of angiogenesis by HGF supplementation has been shown to improve local hypoxia (9, 16, 28, 29). In contrast to other angiogenic factors, HGF has anti-inflammatory and antithrombotic effects (30, 31, 32). HGF is therefore ideal for therapeutic angiogenesis, even under hypoxic conditions such as those that characterize ischemic skin flaps.
However, pharmacokinetic analyses have revealed that the half-life of HGF is short - approximately 4 min. Because the effectiveness of HGF protein therapy might be limited by its short half-life, HGF gene therapy is key to the steady, perioperative release of HGF. Based on our results, delivery of HGF through an adenovirus rather than directly appears to be a feasible and effective treatment option. In our experimental studies, the time frame chosen for injection was 2 days before flap elevation and immediately after flap elevation; this time frame and the dose of HGF were determined on the basis of pilot experiments (data was not shown) and a review of the literature (2, 21). And we confirmed that HGF was expressed from transferred adenovirus by immunofluorescence staining on 10 days after flap elevation. Moreover, the amount of HGF was greater in adenovirus group than in rhHGF group (Fig. 2). We also performed the same experiment with control virus without HGF gene. But, we didn't show the result in this report because it was almost same to the result of the PBS group.
In the present study, flap survival was significantly increased in the HGF virus group compared to the other groups on postoperative days 7 and 10. Although gene transfer of other angiogenic factor such as VEGF, PDGF, and angiopoietin-1 has been shown to improve skin flap survival (33, 34, 35), transfer of the HGF gene into the skin flap via an HGF-expressing adenovirus has not yet been investigated. And we compared the effect of rhHGF and HGF-expressing adenovirus in same study and condition. Thus, we demonstrated that adenovirus-mediated HGF gene therapy in the skin flap increases skin flap viability.
In contrast to the rhHGF group, the HGF virus group showed a significant increase in the numbers of CD31-positive vessels and the expression level of VEGF in skin flap samples taken on postoperative day 10. Furthermore, immunoreactivity for HGF was stronger in the HGF virus group than the rhHGF group. This indicates that the transferred HGF gene had a significant effect on neovascularization. The significant increase in numbers of CD31-positive vessels also indicates that the adenovirus-expressed HGF acted directly on endothelial cells to induce angiogenesis and that it did so more effectively than rhHGF. The increase in intensity of VEGF staining suggests that HGF gene transfer also had a stronger indirect angiogenic effect through the up-regulation of VEGF than rhHGF (13). The significant difference in numbers of CD31-positive vessels and the increased expression level of VEGF on postoperative day 10 in the HGF-expressing adenovirus group suggests that HGF was produced in a sustained way and thereby promoted angiogenesis and induced the production of VEGF until postoperative day 10 in contrast to rhHGF, which had a transient effect.
We observed a significant increase in the ratio of blood flow in the HGF virus group in the mid-distal portion and distal portion of the skin flap until postoperative day 7. Serial measurements of blood perfusion demonstrated that blood flow to the mid-distal portion and distal portion was maintained up to postoperative day 10; in contrast, no blood flow to the skin flap was observed in the other two groups. The maximum time for skin ischemic tolerance in rat, rabbit, and pig skin flaps ranges from 6-13 hr, but it takes longer than this to establish HGF-induced angiogenesis (3). Therefore, the time required for HGF-induced angiogenesis is longer than the critical ischemic time of the skin flap. Overexpression of HGF leads to local blood flow not only by angiogenesis, but also vascular relaxation induced by improvement in endothelial function (36, 37). HGF has been shown to up-regulate VEGF, which is a potent vasodilator that mediates the release of nitric oxide (3, 38). It is therefore likely that the overexpression of HGF by HGF-expressing adenoviruses improved endothelial function and stimulated the production of VEGF followed by vasodilatation within the time frame for skin ischemic tolerance. As a result, the mid-distal and distal portions of the skin flap in the HGF virus group were protected against irreversible ischemic changes and blood flow was maintained. Despite this role, the potential therapeutic use of HGF-expressing adenovirus possesses limitations for safe and effective gene therapy because of acute inflammatory responses and innate immune response. Exhaustive research efforts have prompted the development of novel strategies to overcome these limitations (39). Therefore, we think that further refinement studies will be needed for more efficient and safe gene transfer in patients.
We generated and introduced an HGF-expressing adenovirus (dE1-RGD/lacZ/HGF) into a rat skin flap model. Administration of HGF-expressing adenoviruses into ischemic skin flaps increase skin flap viability, blood flow to the flap, the number of viable capillaries, and VEGF expression, thereby improving the skin flap survival rate.






 XML Download
XML Download