

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With aging, the skin undergoes several changes (1). The collagen production by fibroblasts decreases over time, and this causes thinning of the dermal layer and flattened rete ridges. Dermal elastin and glycosaminoglycans become altered and elasticity diminishes. Subcutaneous tissue diminishes in some areas, especially the face, shins, hands, and feet. As a consequence of these processes facial wrinkles including the nasolabial fold deepens and repetitive movement of facial muscles aggravates these processes.
Because of development of modern medicine, the life expectancy has been extending, and the aged population is increasing. Hence, interest in the reversal of the aging process (anti-aging) has gained more popularity, and the demand on improvement of facial wrinkles is also increasing. In Asia, older people are reluctant to undergo surgery because of their cultural background (2, 3). Furthermore, in Asians, face lifts are often not as effective as in Caucasians because of the thicker skin and wider facial skeleton. Hence, nonsurgical procedures such as thread lifting, subcision, fat grafting and filler injection are preferred (4, 5, 6, 7). While fat grafting has the advantage of being less immunogenic, tissue harvesting often prolongs recovery time, and oil cyst or fibrous tissue replacement may occur over time (8, 9, 10). Compared with fat grafting, filler injection requires only several minutes, and immediate return to social life is possible.
Collagen is the most abundant protein in the body and the first approved filler material for general use by the Food and Drug Administration (FDA) (11). The first collagen filler was made from bovine dermal collagen. Although its effectiveness for the correction of the various wrinkles including the glabellar line, forehead line, and nasolabial fold has been demonstrated, skin testing prior to treatment is recommended because of the risk of developing an allergic reaction (12). In addition, although there has never been a report of prion disease transmission with the use of bovine collagen filler, it has been suggested that the risk of transmission of bovine particles and prions must be considered (13). TheraFill® (SewonCellontech, Ltd, Seoul, Korea) is a newly developed porcine collagen filler that was approved by the Korea Food and Drug Administration (KFDA) for the correction of facial wrinkles. In a preclinical study, TheraFill® demonstrated no evidence of serious complications such as cytotoxicity, allergic reaction, or genotoxicity. Moreover, it does not require skin testing.
The aim of the present study was to compare the 12-month efficacy and safety of a porcine collagen filler (TheraFill®) with that of a bovine dermal collagen filler (KOKEN®, Koken Co., Ltd., Tokyo, Japan) for nasolabial fold correction.
MATERIALS AND METHODS
Materials
TheraFill® is a 3% gel suspension of porcine collagen Type I plus 0.3% of lidocaine in phosphate-buffered physiologic saline that was delivered in a disposable 1 mL syringe with 27-gauge needle. It is prepared by a process that includes enzymatic digestion to remove the antigenic portion of the molecule, making it immunologically compatible with humans. KOKEN® is a 3.5% gel suspension of bovine collagen that was delivered in a disposable 1 mL syringe.
Subject selection and study design
This randomized, double blinded (subject and evaluator), split-face non-inferiority study was conducted at 2 hospitals (Seoul St. Mary's Hospital and Bucheon St. Mary's Hospital) in Korea. Adult (>20 yr) subjects of either sex with mild to severe nasolabial folds based on 5-point Wrinkle Severity Rating Scale (WSRS) (none, 1; mild, 2; moderate, 3; severe, 4; extreme, 5) were included. The exclusion criteria were experience of a nasolabial fold correctional procedure such as botulinum toxin injection, filler injection, laser or chemical peeling, or face-lift within 6 months before this study. Subjects with a history of hypersensitivity to injectable collagen, severe allergic reaction, autoimmune disease, and connective tissue disease, and a current skin disease or inflammation in the nasolabial fold area were also excluded. Two treating investigators, one at each hospital, treated the subjects. Before starting the study, they were trained to ensure the use of the same technique. Firstly, a topical anesthetic cream was applied 30 min before the procedure, after which sterile draping was performed using 75% alcohol. Needle was inserted at the lowest part of the nasolabial fold and advanced along the fold. In the highest part of the fold, the triangular depression was corrected using the fan technique, after which the needle was retreated downward and collagen was injected using the linear technique. The needle stayed within the dermal layer, specifically at the mid-dermal level in the upper fold and at the mid- to upper-dermal level in the lower fold. For over-injected or under-injected areas, massage was performed to evenly distribute the collagen. At initial screening, all eligible subjects received a collagen test injection in the dermis to assess their sensitivity to bovine collagen. Subjects who showed hypersensitivity reaction were excluded from this study. Each subject received TheraFill® in one nasolabial fold and KOKEN® on the contralateral side. Treatments were randomly allocated using a computer-generated code. During injection, the subjects were blinded to the treatment by wearing eye shields or concealing the syringe.
The response to the initial injection of either filler was evaluated after 2 weeks, and if the result was considered suboptimal, one "touch-up" treatment was performed to achieve "optimal cosmetic result" (OCR). Subjects were followed up at 3 month intervals over a 12-month period after OCR achievement.
The 3 evaluating investigators who were unaware of the treatment allocation assessed the efficacy of eachfiller by reviewing photographs taken at each follow-up. Investigators assessed the efficacy by using the 5-point WSRS. The degree of overall improvement was determined at each visit by the same investigators and the subjects using the Global Aesthetic Improvement Scale (GAIS) (5, very much improved; 4, much improved; 3, improved; 2, no change; 1, worse). The pretreatment photography served as the reference image at each follow-up visit.
Subjects were surveyed about adverse events. They were asked to describe any subjective discomfort that they felt on the site of injection. Injection sites were examined for evidence of edema, erythema, induration, pain, bruise, nodule, infection, or inflammation at every visit. Adverse reactions were kept in record and followed up for changes. If an inflammatory reaction occurred, laboratory tests including immunoglobulin assay were performedat the investigator's discretion.
Statistical analysis
The primary efficacy endpoint was the WSRS score at 12 month post-baseline. The non-inferiority analysis of the within-subject difference from screening in WSRS was performed by constructing the 90% two-sided confidence interval on the within-subject difference between TheraFill® and KOKEN®. If the lower limit of this interval was greater than -0.5, then TheraFill® was considered non-inferior in efficacy to KOKEN®. The secondary efficacy endpoints included followings: 1) WSRS scores at each visit; 2) investigator- and subject-assessed GAIS at each visit. The paired t-test was used to analyze secondary endpoints and a P value less than 0.05 was considered to be statistically significant.
RESULTS
Subjects demographics
Of the 61 subjects who were treated, 57 subjects (53 females and 4 males) completed 12 months of follow-up. The causes of withdrawal were consent withdrawal (1) and loss to follow-up (3). The mean age of the subjects was 47.2 yr. Regarding age distribution 24 (42.1%), 16 (28.1%), 11 (19.3%), and 6 (10.5%) were in their forties, fifties, thirties, and sixties, respectively.
Efficacy
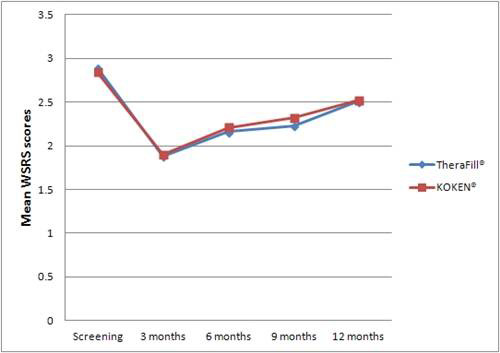
The mean volume of the filler did not significantly differ between the groups: 2.11±0.60 mL in the TheraFill® group and 2.17±0.43 mL in the KOKEN® group. The mean WSRS scores before treatment were 2.89±0.7 in the TheraFill® group, and 2.84±0.7 in the KOKEN® group (P=0.322). At each follow-up, the mean WSRS scores were 1.88±0.84 (3 months), 2.16±0.7 (6 months), 2.23±0.66 (9 months), and 2.51±0.71 (12 months) in the TheraFill ® group. For the KOKEN® group, the score were 1.90±0.97 (3 months), 2.21±0.67 (6 months), 2.32±0.60 (9 months) and 2.52±0.60 (12 months) (Fig. 1A). The lower limit of the two-sided 90% confidence interval was -0.0312, which was above the predefined margin for non-inferiority (-0.05). This indicates that the efficacy of TheraFill® at 12 month post-baseline was comparable to that of KOKEN®. Although, there was a slightly higher improvement in WSRS scores in the TheraFill® group at each follow up, the difference between both groups was not statistically significant. Regarding the GAIS assessment by the investigators, the mean scores at each follow up were 3.42±0.63 (3 months), 3.05±0.85 (6 months), 2.63±0.82 (9 months), and 2.28±0.82 (12 months) in the TheraFill® group and 3.3±0.76 (3 months), 3.11±0.84 (6 months), 2.72±0.82 (9 months), and 2.26±0.84 (12 months) in the KOKEN® group (Fig. 1B). GAIS assessment by subjects showed that the mean scores were 3.54±0.83 (3 months), 2.98±0.92 (6 months), 2.61±0.88 (9 months), and 2.28±0.67 (12 months) in the TheraFill® group and 3.47±0.95 (3 months), 2.98±0.88 (6 months), 2.65±0.81 (9 months), and 2.33±0.81 (12 months) in the KOKEN® group (Fig. 1C). The mean GAIS score decreased significantly from 6 months in both groups (P<0.001). There was no significant difference between the 2 fillers at any of these time points. Serial photographic images of the nasolabial folds are presented in Fig. 2.
Safety
Both fillers were well tolerated and there were no serious adverse reactions. In the TheraFill® group, swelling at the injection site occurred in 1 subject. In the KOKEN® group, 5 adverse reactions occurred in 3 subjects and swelling (n=3) was the most common local side effect, followed by erythema (n=1), and nodule (n=1). All of the side effects were mild in intensity, and were resolved without sequelae.
DISCUSSION
During a lifetime, structural proteins in the skin undergo changes. With aging, the collagen production by fibroblasts is decreased and the collagen bundles are fragmented. The level of collagenase is increased by ultraviolet radiation and degradation of collagen is fastened. As a consequence of these changes, dermal thickness in aged skin is decreased by 20% (14, 15).
Reversal of the skin aging process by soft tissue augmentation has been of great interest to physicians as well as the general population. In particular, because of the collagen defects in aged skin, several studies on collagen as a dermal filler have been performed (12, 16). Zyderm I® (Allergan, Inc, Irvine, CA, USA) a purified suspension of bovine collagen, was the first dermal filler available for the correction of wrinkles and was approved by the FDA in 1981. It is composed of 3.5% bovine dermal collagen, suspended in physiologic phosphate-buffered sodium chloride solution and 0.3% lidocaine. Since then, Zyderm II® (Allergan, Inc, Irvine, CA), which contains 6.5% bovine dermal collagen, and Zyplast® (Allergan, Inc., Irvine, CA, USA), which contains 3.5% bovine dermal collagen cross linked with 0.0075% glutaraldehyde were approved in 1983 and 1985, respectively. Because collagen fillers are natural and dermal filling with collagen is performed according to the principle of "replace like with like", bovine collagen came to be regarded as the "gold standard" among injectable fillers (17). However, immunogenicity and potential hypersensitivity reactions have decreased the popularity of bovine collagen fillers. It has been demonstrated that approximately 3%-3.5% of subjects will show sensitivity; therefore, 2 consecutive skin tests are recommended (6 and 2 weeks) prior to treatment (18). In addition, the risk of xenogenic transmission of BSE is not eliminated.
Due to its high biocompatibility with humans, porcine collagen has been used in various clinical fields including abdominal wall surgery, orthopedic surgery, and gynecologic surgery (19, 20, 21). Recently, it has been demonstrated that porcine-based dermal collagen filler is effective for the treatment of facial wrinkles including the nasolabial fold and tear-trough deformity (22, 23). In addition, Lorenc et al showed that porcine collagen filler provided a lower extrusion force and yield point compared with hyaluronic acid-based fillers (24). These physical properties of porcine collagen filler allow clinicians to inject more comfortably and precisely. TheraFill® is a newly developed porcine collagen filler from South Korea. By enzymatic digestion of immunogenic telopeptides, the issues regarding xenogenic allergy are resolved and skin test prior to injection is not needed. Furthermore, patients feel free from xenogenic transmission of BSE. In our study, there were no serious or long-lasting complications including allergic reaction. However,a previous study has reported that Evolence®, a cross-linked porcine-based collagen filler, should not be injected into the lips due to the high incidence of nodule formation (25). For this reason, it seems prudent to investigate the safety of TheraFill® through further studies on other facial areas. Regarding efficacy, the WSRS data of TheraFill® at 12 month post-baseline was comparable to that of KOKEN®. In addition, there was no significant difference in the efficacy of between TheraFill® and KOKEN® during 12 months after the injection. However, regarding durability, GAIS score decreased significantly from 6 month in both groups. This is due to the degradation of natural collagen by in vivo collagenase and is consistent with the results of previous studies, which showed that the majority of subjects require touch-up injections approximately every 3-12 months (26, 27). A previous study has reported that ribose-induced cross linking of porcine collagen prolongs the effect of collagen filler (28). In addition, it has been demonstrated that cross-linked collagen filler has comparable efficacy for treating nasolabial fold to hyaluronic acid based filler (22). Therefore, it seems that further development such as increasing the degree of the cross link or concentration of collagen is needed to improve the current form of TheraFill®.
In conclusion, the long-term effect of TheraFill® on nasolabial fold correction was comparable to that of the bovine collagen filler. Regarding safety, it was tolerable in most cases, and there was no serious adverse reaction. Therefore, TheraFill® may be a good alternative to bovine collagen fillers. Further studies are needed to compare its safety and efficacy with those of widely used hyaluronic acid-based filler.


 XML Download
XML Download