

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The one-year mortality of hip fractures in elderly patients ranges from 14%-36%, and the incidence of hip fractures is increasing each year because of increasing the number of the elderly. Epidemiologic studies on hip fracture in Korea have reported high incidences of hip fracture, and confirmed that the number of hip fractures is likely to increase markedly in the near future (1, 2). It is a worldwide problem related to the aging of the population (3, 4, 5, 6, 7). It is expected that 63 million hip fractures will occur globally in 2050; and Melton et al. reported 6% of males and 17.5% of females will experience hip fracture (3, 4). The complications of hip fracture are death, disability, long term care needs and loss of social independency (8). Thus hip fracture appears as a significant public health problem with serious socioeconomic burden (9). Hodsman et al. (5) reported that patients with previous hip fractures will experience subsequent hip fractures (SHF) and they also suggested that the mortality is 2.7 times higher than the group without previous fractures. The incidence of asynchronous bilateral hip fractures is 1.7%-14.8%; and hip fractures alone are a major risk of contralateral fracture (10, 11, 12, 13, 14, 15, 16, 17). So we analyzed the incidence of subsequent hip fractures and its risk factors in the northwestern region of Korea.
All hip fracture patients (femoral head fractures, femoral neck fractures, intertrochanteric fractures, subtrochanteric fractures) treated at teaching 5 hospitals in Bucheon and Incheon area were reviewed. The patients were divided into two groups, a group that had experienced subsequent hip fractures (SHF), and a group that had unilateral hip fractures (UHF). We analyzed the incidence of SHF and the risk factors of SHF.
MATERIALS AND METHODS
We analyzed 2,546 patients (female, 1,770; male, 776). Inclusion criteria were patients who had unilateral hip fracture from January 2000 to December 2010 with no osteoporosis treatment at the time of the incident. Exclusion criteria were patients who received osteoporosis treatment at the time of the incident and causes of hip fracture were a traffic accident, a fall from a higher pointer than the patient's height, pathologic fracture and causes of follw-up loss were unknown. The average follow-up period was 12 months (1-130 months). Presence of SHF, alcohol history, marital status, dementia, dizziness, osteoporosis treatment after fracture, American society of anesthesiologists (ASA) score, body mass index (BMI) and bone mineral density (BMD) were collected through patients' medical records and telephone interviews. Patient identification (using name and birth date) was cross checked between hospitals to obtain an accurate count of incidence. We selected a SHF group with a previous history of surgery due to unilateral hip fracture and who had SHF on the contralateral side. BMD tests were performed on 1,421 patients after inital trauma with Dual-energy X-ray absorptiometry. Student's t-tests and chi-square test were performed between the two groups on their age, BMI, BMD and ASA score. We analyzed the factors known to cause SHF such as additional fractures, alcohol consumption, solitude habitation, dementia, dizziness, medical condition, and history of osteoporosis treatment by logistic regression analysis (SPSS 18.0).
RESULTS
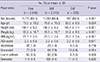
Their average age was 79.2 (range: 50-100 yr) yr with 776 males and 1,770 females. Seventy-one (2.8%) patients were died. Average BMI was 23.1. Alcoholism was noted in 26 patients (1%). Sixty-three patients (2.5%) lived in solitude. One hundred thirteen patients (4.4%) suffered from dementia. Their ASA physical status scored 2.3 (1-4, standard deviation [SD] 0.5) on average. Two hundred thirty three patients (9.2%) experienced a SHF. Average interval between the first fracture and the subsequent hip fractures was 30.2 months (range, 4 days-154 months). There were 3 (1.3%) alcoholism cases with SHF, 3 (1.3%) lived in solitude, 11 (4.7%) had dementia. Their ASA physical status score was 2.3 (1-4, SD 0.5) on average. In the group with UHF, 60 cases (2.6%) lived in solitude, 102 cases (4.4%) had dementia, 23 (1%) alcoholism cases. Their ASA physical status score was 2.3 (1-4, SD 0.5) on average. The two groups had statistical differences in sex, age, BMI and marital status (Table 1).
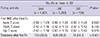
T-scores at the time of initial trauma were -2.89 (SD 1.09) of femoral neck area and -2.42 (SD 1.16) of trochanteric area. A total of 703 patients (49.5%) received osteoporosis treatment after the initial fracture. A total of 138 patients with SHF had a T-score of -2.83 (SD 1.43) of femoral neck area, and -2.37 (SD 1.43) of trochanteric area, and 1,283 patients with UHF had a T-score of -2.89 (SD 1.05) of femoral neck, and -2.42 (SD 1.13) of trochanteric area. An initial T-score in the group with SHF was -2.83 (SD 1.43) while group with UHF showed a T-score of -2.89 (SD 1.05), thus showing no statistical difference (P=0.643). However, more patients in the SHF group had been receiving treatment for osteoporosis (P<0.001) (Table 2).
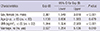
In this study, overall incidence of subsequent hip fractures was 9.2%. Multivariate analysis of risk factors found that female gender, BMI<22 kg/m2, being unmarried were statistically significant risk factors (Table 3).
DISCUSSION
The occurrence of fracture near the hip joint is increasing as our average life span increases due to medical improvement. However, mortality rates and complication rates are very high regardless of technological advances (18, 19). Boston (16) reported that in the cases of a first femoral neck fracture, death rate goes up to 13% and 30% in cases of a second fracture. Common risk factors for hip fractures are low BMI and small calcium intake in Japan and Mediterranean osteoporosis study (MEDOS). Additionally eating fish and sleeping on Japanese mattress might exert preventive effects against hip fracture (20). The risk factors of bilateral hip fractures are dementia, neurological diseases, and Parkinson disease (10, 12, 21). Denutrition is also a risk factor (22, 23). In this study, female gender, BMI<22 kg/m2, being unmarried were found as risk factors.
Our study has some limitations. This was a multicenter study and the prescription and duration of osteoporosis medication differed between centers. Therefore the effect of medication on SHF was difficult to estimate. Second, because a number of different surgeons were included in the study, the incidence depending on operative procedures was difficult to evaluate. Third, being a retrospective study, the collection of data was irregular and BMD tests were performed on only 1,421 patients after initial trauma, not all patients. Fourth, investigation of patients' calcium profiles, hormonal status, vitamin D deficiency was not performed.
However, this is a substantially large study that included all of the teaching hospitals in the Incheon and Bucheon area. Patient identification was cross checked between hospitals leading to an accurate evaluation of the SHF patients in the community.
In this large-scale, retrospective, multicenter study, overall incidence of subsequent hip fractures is 9.2%. Independent risk factors of subsequent fracture are female gender, BMI<22 kg/m2, and being unmarried.
 XML Download
XML Download