

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebrovascular disease is the second leading cause of death and the major cause of disability in Korea (1). Each year, about 105,000 Koreans experience a new or recurrent stroke and this number is estimated to rise up to 350,000 by 2030 (2). It has been considered that stroke frequently affects the elderly aged 55 yr or older, and rarely affects young adults aged between 15 and 45 yr (3, 4, 5, 6). Recent studies provide evidence that ischemic stroke in young adults is increasing worldwide (1). Although both prognosis and outcome of young adults stroke patients are better than those observed in older patients, stroke in younger adults has greater socioeconomic burden and quality of life consequences due to its longer duration than stroke in older adults (4, 7). Moreover, there are differences in etiologic and prognostic factors between young and old age stroke (6, 8).
Until now, numerous studies have been conducted to identify etiology, risk factors, and prognostic factors of stroke in young adults, but most of these studies have been conducted in a single-institutional setting with small sample sizes (4, 5, 9, 10). Furthermore, most of these studies have examined both hemorrhagic stroke and ischemic stroke, and only few studies have compared the epidemiologic features, emergency care, and outcomes between young adults and the elderly.
The objective of the present study was to examine demographics, epidemiologic features, emergency care, and outcomes of ischemic stroke in two age groups, young adults and the elderly in Korea.
MATERIALS AND METHODS
Study setting and data sources
We used the data from the Cardiovascular Disease Surveillance (CAVAS) Project, which was a hospital-based registry from 29 tertiary teaching hospital emergency departments (ED) in Korea during November 2007 to October 2010. The CAVAS project, supported by Korea Centers for Disease Control and Prevention (CDC), collected information on patients with acute myocardial infarction (AMI) (ST elevation MI and non-ST elevation MI) and all stroke (ischemic stroke, hemorrhagic stroke, and subarachnoid hemorrhage) within 1 week of disease onset. Participating hospitals were tertiary and teaching hospitals located in metropolitan or urban areas. All hospitals provided 24 hr/7 days emergency cardiac and stroke care by emergency physicians and cardiovascular/neurovascular specialty doctors (11).
Study subjects
Ischemic stroke patients who were diagnosed at study hospitals were included in the present study. The definition of ischemic stroke was defined based on the international classification of disease 10th version (ICD-10) codes. Ischemic stroke patients were included if they had one of following ICD-10 diagnosis codes; I60.0-I60.9, I61.0-I61.9, I63.0-I63.9, and I64. We excluded patients with less than 15 yr of age or without information on age and confirmed diagnosis code.
Data variables and data collection
Data variables included demographics (age and gender), socioeconomic factors (type of insurance, education level, and occupation), time variables related with event and process of care (time of event, prehospital care, ED care, and hospitalization), clinical parameters, laboratory and radiologic examinations, and emergency care procedures (prehospital care, interhospital transport, and hospital care). Primary endpoint was hospital mortality at discharge. Secondary endpoint was disability at discharge measured by modified Rankin Scale (ranged from 0 (no disability) to 6 [fatal]). For each patient, both pre-event and discharge modified Rankin Scale were measured.
Information was collected by study hospital staffs, such as nurse, emergency medical technicians, interns, residents, and attending physicians according to hospital specific human resources. Hospital care and outcomes were recorded by trained study coordinators, who were employed by each ED and reviewed medical records for hospital outcomes. The collected information was then imported to a database via a web-based data entry operated by Korea CDC. Regular quality management process was performed by the central data quality control committee, composed of emergency physicians, cardiologists, and neurologists, epidemiologists, and biostatisticians. Regular education and training were provided to maintain the data quality collected by study coordinators. All education and training were performed using a designed data collection instruction with various case examples.
Statistical analysis
We categorized the patients into two age groups; young adults (15-45 yr) and elderly (46 yr and older). We compared the demographics, epidemiologic features of risk factors, emergency care, and hospital outcomes. Continuous variables were described with mean (standard deviation) and median (interquartile range). Categorical variables were described with frequency and percent. Categorical variables were analyzed using chi-square-test and continuous variables were analyzed using Mann-Whitney U test and Student's t-test. Statistical analysis was done using PASW for Windows 21.0 (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered statistically significant.
RESULTS
Patient characteristics
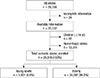
During the study period, a total of 39,156 patients visited the participating EDs due to acute stroke. Of these, patients with incomplete information (n=24), hemorrhagic stroke (n=13,314), and children age less than 14 yr old (n=92) were excluded. Total 25,818 patients were analyzed (young adult 5.5% and elderly 94.5%) (Fig. 1).
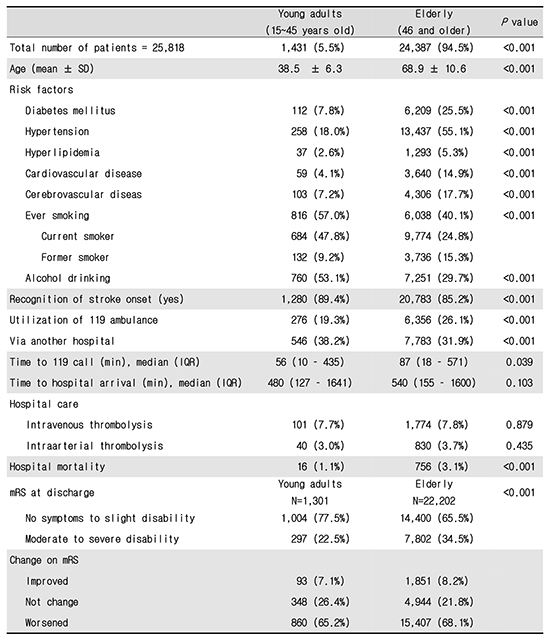
Comparison of demographic findings
Compared to elderly, young adults ischemic stroke showed significantly higher proportions of being male, having high body mass index, better socioeconomic status such as higher education level, professional and business job category, and national health insurance program (P<0.001 for all). The number of patients with traditional risk factors of developing stroke, such as diabetes mellitus, hypertension, and hyperlipidemia, was significantly higher in elderly compared to young adults; 25.5% vs. 7.8% for diabetes mellitus, 55.1% vs. 18.5% for hypertension, and 5.3% vs. 2.6% for hyperlipidemia. In addition, the number of patients with past history of cardiovascular and cerebrovascular diseases was significantly higher in elderly than young adults (P<0.001). On the other hand, compared to elderly, significantly higher proportion of young adults were exercising, smoking, and consuming alcohol. Primary symptoms, including mental change, sensory abnormality, unable to walk, and dizziness were significantly different between two age groups (Table 1).
Emergency care and process
Young adults ischemic stroke showed less utilization of emergency medical services (EMS) while the time to call for ambulance was significantly shorter in young adults than the elderly (56 min vs. 87 min, P=0.039). Time from symptom onset to hospital arrival was similar between two groups (P=0.103). Young adults were more likely to be transported from another hospital than the elderly. Time interval between ED arrival and brain CT scan was shorter in the elderly than young adults (30 vs. 33 min, P<0.015). The number of patients receiving reperfusion therapy was not different between two groups while operation rate was higher in young adults (Table 2).
Hospital outcomes and disability
Overall hospital mortality was higher in the elderly than young adults (3.1% vs. 1.1%, P<0.001). However, hospital length of stay was not different between two groups (Table 3). The modified Rankin Scale (mRS) before the event was higher in the elderly compared to young adults with 9.4% and 3.3% of the elderly and young adults were in the moderate to severe disability category, respectively (P<0.001). Moreover, more elderly patients showed worsen change of mRS before and after the occurrence of stroke compared to young adults (68.1% vs. 65.2%, P<0.001) (Table 4).
DISCUSSION
The present study from a large nationwide multi-center hospital-based cardiovascular registration compares demographic, epidemiological, emergency care, and hospital outcomes between young adults and elderly ischemic stroke.
Our results showed that young age ischemic stroke accounted for 5.5% of total ischemic stroke patients, which is greater than 3.7% on the National Survey of Stroke in North America (3), but lower than 8.5% reported by Bevan et al. (4). Previous studies on stroke in young adults in Korean population have reported the proportion of stroke in young adults as about 14%, which was much higher than the incidence observed in our study (9, 10). This might be because the current study was a multi-center study while previous studies were single institution reports. Also, the patients with ischemic stroke in young age group accounted for 38.5% of all kinds of stroke in the current study. Although this value was close to 41% reported by Bevan et al., it was greater than 31.9% and 30.5% reported by two previous studies in Korean population (9, 10). It is well known that intracerebral hemorrhage and subarachnoid hemorrhage occur more frequently than cerebral infarction in young adults unlike in the elderly (12, 13). However, a recent study by George et al. reported that there is an increasing tendency in the rate of hospitalization in young adults with acute ischemic stroke (14).
One study which examined trends in the incidence of stroke during a period from 1993 to 2005, reported that while there was a decrease in the overall incidence of stroke, the proportion of stroke in young adults (age range: 20-54 yr) increased from 12.9% to 18.6% (15). According to this report, this increase in trend was associated with the increase in the prevalence of diabetes mellitus, hyperlipidemia, and obesity among young adults, which are major risk factors for stroke. A numerous studies have shown that the prevalence of stroke increases with the increased incidence of hyperlipidemia, obesity and diabetes mellitus in young adults (8, 14). Also in Korea, the prevalence of these diseases has been gradually increasing (2, 16, 17). Therefore, the resulting increase in the prevalence of stroke is one of major public health concerns. Although it is known that most risk factors for stroke increase with age, the main objective of our study was to evaluate and compare the distributions of these risk factors in young adults and the elders. In the present study, we demonstrated the difference in the risk factors in two different age groups using a multi-center registry.
In addition, our results demonstrated that the proportions of smokers and alcohol drinkers were significantly higher in young adults than in the elderly. The smoking is one of the major risk factors of developing stroke through vasoconstriction, platelet aggregation, elevation of blood coagulation factors, increased blood viscosity and elevated blood pressure (18, 19). Although there has been a decreasing tendency in the smoking rate since 1998, Korea still shows a high smoking rate. Currently, about 48.3% of Korean adult males aged 19 yr or older are smokers and Korea ranks the 5th in smoking among the Organization for Economic Co-operation and Development (OECD) countries (17, 20). In particular, the age-specific smoking rates in the 20s, 30s and 40s were estimated to be 47.3%, 60.9% and 53.6%, respectively (17). In this study, the significantly higher proportion of ever-smokers in young adults compared to the elderly was even higher when only current smokers were compared. Numerous studies reported that smoking was the important risk factor for stroke in young adults with dose-response relationship between cigarette smoking and risk of ischemic stroke (18, 21, 22). The alcohol drinking is also involved in the occurrence of stroke through various mechanisms. Alcohol increases risks of developing cerebral embolism by causing cardiac arrhythmia and cardiac wall dysfunction, elevates the blood pressure, promotes the platelet aggregation and blood coagulation, induces the contraction of cerebrovascular smooth muscle cells and thereby decreases the cerebral perfusion and alters the brain metabolism (23). According to a Finnish study conducted by Hillbom and Kaste, ethanol intoxication was preceded in 40% of total patients within 24 hr before the onset of stroke (24). The proportion of alcohol drinkers in young adults was 54.9% in our study, showing that the alcohol drinking was the most prevalent risk factor in young adults.
Several studies had shown that the proportion of patients with stroke receiving definitive treatments such as thrombolytic agents was significantly increased because the pre-hospital and in-hospital period was significantly shortened if they used emergency medical system (25, 26). However, in this study, the proportion of young adults who visited the first hospital using 119 ambulances was smaller than that of the elderly, and therefore, young adults were more likely to be transported from another hospital than elderly. Moreover, only 29.8% of young adults with ischemic stroke reached hospital within three hours of onset of stroke symptoms during which they were allowed to receive thrombolytic agents, and the median elapsed time between the onset of symptoms and hospital arrival was 480 min. Because proportion of patients with known time of symptom onset was higher in young adults than elders, young adults had shorter median symptom onset to hospital arrival time. However, they used 119 ambulances less frequently than elders, thus more likely to visit the primary or secondary hospital first, where definitive treatments cannot be provided, and more likely to be transferred to the tertiary hospital than elders. These are very important factors in the aspects of treatment results and prognosis.
Our study showed better hospital outcomes in young adults than the elderly as shown in other previous studies. While overall mortality was very low in young adults (1.1%), 22.5% of them were remained to have moderate to severe disability and 65.2% of them were shown to have worsened disability suggesting that young age stroke can make huge economic burden. Hospital length of stay was not different between young adults and elderly group. If young adults can receive better systems of stroke care program, such as higher proportion of ambulance utilization and shorter time interval to definite care, then the full recovery discharge will increase.
Although this is one of the largest ED-based studies, there are a number of limitations. First, the participated emergency departments were located in either metropolitan or urban areas, where more resources were allocated than other parts of the country. If smaller hospitals in rural areas participated in the study, the results might have been changed. Second, we could not clarify effects of underlying conditions such as congenital cardiac anomaly or cerebral vascular anomaly, which were known to be responsible for the occurrence of stroke in young adults. Third, we did not compare the effect size of the risk factors on outcomes, but just compared the distributions between two age groups. If we adjust for confounders, effect of age group on hospital outcomes and disability might be different than what we observed in this study. Last, we used the cut off age of 15 to 45 for young adults based on the cut-point used in previous studies. However exact age criteria were not decided in most studies (3, 4, 5, 9, 10).
From ED-based stroke registry, young adults stroke showed very different epidemiologic features when compared with elderly patients. In young adults, overall hospital mortality was 1.1% and moderate to severe disability at discharge as measured by mRS was about 22.5%. For developing prevention program for young adults stroke, further studies should be investigated to determine the association between stroke risk factors and outcomes.



 XML Download
XML Download