

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gliomas are the most frequently occurring malignant primary brain tumors in adults (1, 2, 3, 4). Since the 1940s, chemotherapeutic agents have been used increasingly for the treatment of various types of brain tumors. Despite multimodality treatments, the outcome of patients with glioma remains poor.
Temozolomide has been used in the treatment of glioma and it has been shown to improve the outcomes (5). Temozolomide is an orally administered chemotherapeutic drug that methylates DNA in a way that prevents tumor cell proliferation. Temozolomide is a second-generation alkylating agent approved by the Food and Drug Administration in 1999 (1, 2, 5). After Stupp et al. reported the efficacy and toxicity of temozolomide, it became a popular and standard regimen in the chemotherapy of malignant gliomas (2). Since 2006, it has been approved for the standard treatment of newly diagnosed glioblastoma in conjunction with radiotherapy in Korea.
Although temozolomide was proven effective at increasing longevity, quality of life is another important consideration in patients with gliomas. Toxicity from temozolomide has the potential to negatively impact patient quality of life. Some authors in previous papers have reported several toxicities of temozolomide (2, 6, 7, 8), but their studies were simple and limited and had a greater emphasis on the efficacy of temozolomide. Therefore, we focused primarily on the toxicity and safety of temozolomide. We investigated common temozolomide side effects and any fatal side effects associated with temozolomide use. In addition, nursing care strategies were proposed for decreasing temozolomide toxicity and for increasing the quality of life of malignant glioma patients.
MATERIALS AND METHODS
Patients
A total of 347 patients with malignant gliomas underwent temozolomide therapy at two hospitals of Seoul National University between 2004 and 2010. The 4 selection criteria of this study were as follows: patients aged over 17 yr; histologically confirmed WHO grade 3 or 4 gliomas; patients treated with temozolomide as a concomitant, adjuvant or palliative method; and available complete medical records regarding the toxicity of temozolomide. Consequently, 300 patients were retrospectively reviewed in this study.
The demographic data of the reviewed 300 patients are summarized in Table 1; 187 patients (62.3%) were male, and 113 patients (37.7%) were female. The patient median age was 49 yr (range, 17-84 yr). The body surface area ranged from 1.27-2.16 m2 (median, 1.72 m2). Before temozolomide was administered, 205 patients (68.3%) showed a Karnofsky performance score (KPS) greater than 80.
The most common pathology was glioblastoma (n=210; 70%) followed by anaplastic astrocytoma (n=40; 13.3%) and anaplastic oligodendroglioma (n=16; 5.3%). Concurrent chemoradiotherapy (CCRT) treatment (75 mg/m2/day×42 days) only was administered to 46 patients (15.3%), and 162 patients (54.0%) received adjuvant treatment only (150-200 mg/m2/day for days 1-5 every 28 days). CCRT and subsequent adjuvant treatment were administered to 92 patients (30.7%). Therefore, 138 patients received temozolomide as CCRT, and 254 patients received it as an adjuvant treatment.
Toxicity assessment
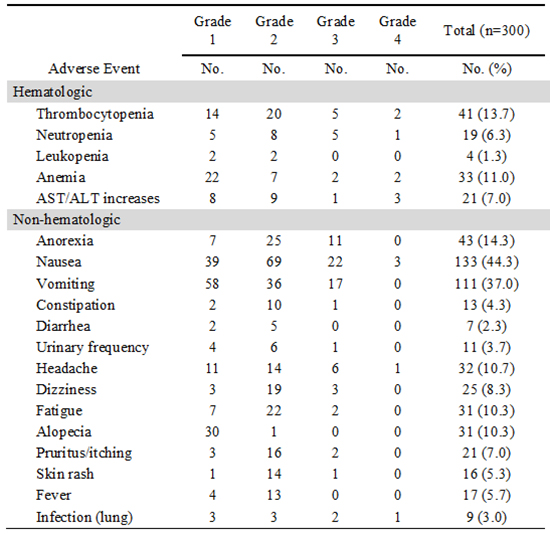
The severities of the toxicities were assessed by oncologists at the two medical centers using the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 developed by the National Cancer Institute. In the CTCAE, a score of 1 indicates mild adverse effects, a score of 2 moderate adverse effects, a score 3 severe adverse effects and a score of 4 life-threatening adverse effects (9). Hematologic toxicities, including thrombocytopenia, neutropenia, leukopenia, anemia and AST/ALT increases were assessed. Among non-hematologic toxicities, anorexia, nausea, vomiting, constipation, diarrhea, urinary frequency, headache, dizziness, fatigue, alopecia, pruritus/itching, skin rash, fever and lung infection were assessed.
Statistical analysis
The data are expressed as the median value and range. Using Pearson's chi-square test toxicity differences were compared by patients' characteristics: gender; age of ≥70 and <70 yr; KPS score of ≥70 and <70; and histologic grade of 3 and 4. The chi-square test was also performed to evaluate toxicity differences between CCRT and adjuvant treatments. The limit of significance was 0.05 (two-sided) in all analyses. All statistical analyses were performed using the SPSS statistical software package (version 17.0.1, 2008; SPSS, Chicago, IL, USA).
RESULTS
Treatment intensity
Table 2 shows the intensity of the treatment administered to the 300 patients. The duration of therapy ranged from 13-58 days (median, 42) in the 138 patients treated with CCRT. A total of 110 patients (79.7%) were treated with ≥90% of the planned dose, while 28 patients (20.3%) discontinued temozolomide. Adjuvant therapy was administered to 254 patients. The number of temozolomide cycles ranged from 1-19 (median, 7). Total 115 patients (45.3%) completed 6 cycles, and 139 patients (54.7%) could not complete 6 cycles.
Overall toxicity profile with temozolomide
A total of 209 patients (69.7%) reported 618 toxicities (Table 3). In this study, 255 toxicities (36.4%) were CTCAE grade 1, 299 (48.4%) were grade 2, 81 (13.1%) were grade 3, and 13 (2.1%) were grade 4. The number of hematologic toxicities was 118, including thrombocytopenia (n=41, 13.7%), anemia (n=33, 11.0%), increased AST/ALT (n=21, 7.0%) and neutropenia (n=19, 6.3%). Non-hematologic toxicities were more common. One hundred thirty-three patients (44.3%) suffered from nausea, 111 patients (37.0%) from vomiting, 43 patients (14.3%) from anorexia, 32 patients (10.7%) from headache, 31 patients (10.3%) from fatigue and 31 patients (10.3%) from alopecia. None of our patients presented with fatal Pneumocystis jiroveci pneumonitis. There was no mortality due to temozolomide. We observed 4 patients (1.3%) with leukopenia.
Management of temozolomide toxicity
The most common toxicities with temozolomide were gastrointestinal troubles, such as nausea, vomiting and anorexia. Anti-emetics were administered to 179 patients (73.4%) out of 244 patients who experienced nausea and vomiting. To mitigate gastrointestinal troubles, two anti-emetics, 5-HT3 receptor antagonists (ondansetron, ramosetron, granisetron, dolasetron, or tropisetron) and dopamine receptor antagonists (metoclopramide) were administered separately or in combination: 5-HT3 receptor antagonists only, 74 patients (41.3%); dopamine receptor antagonists only, 51 patients (28.5%); and 5-HT3 receptor antagonists and dopamine receptor antagonists in combination, 54 patients (30.2%). When hematological toxicities, such as leukopenia, thrombocytopenia and anemia occurred, the delay or discontinuation of temozolomide therapy was decided by the physician.
Comparison of toxicities by patients' characteristics
The differences in the temozolomide toxicity profile by characteristics such as gender, age, KPS score and histologic grade were assessed. There were no significant differences in toxicities by characteristics but by gender. Only thrombocytopenia (P=0.002) and vomiting (P=0.048) were more common in female than in male.
Comparison of toxicities between CCRT and adjuvant treatment
The differences in the temozolomide toxicity profile between the CCRT and adjuvant treatment groups were assessed (Table 4). Hematologic toxicities were more likely to develop in CCRT-treated patients. The proportion of neutropenia, anemia and AST/ALT increases was significantly higher in CCRT-treated patients than in adjuvant-treated patients (P<0.05). Of the non-hematologic toxicities, anorexia, alopecia, pruritus/itching, skin rash and lung infection were significantly more common in CCRT-treated patients, while diarrhea and headache were more common in adjuvant-treated patients (P<0.05).
DISCUSSION
We thoroughly evaluated the toxicity profile of temozolomide in the 300 patients diagnosed with malignant gliomas. Although temozolomide showed many types of toxicities, 84.8% of the toxicities were grade 1 or 2 and were tolerable to patients. However, gastrointestinal troubles, such as nausea (44.3%) and vomiting (37.0%), were exceedingly common. Nausea and vomiting are known as two of the most common, disturbing, and potentially serious side effects of chemotherapy and have physically and emotionally adverse effects on the quality of life of patients with cancer (10, 11). This may require physicians and nurses to carry out aggressive monitoring of gastrointestinal toxicities and to administer prophylactic anti-emetics. In addition, relatively common hematologic complications, including thrombocytopenia (13.7%) and anemia (11.0%), should also be carefully monitored.
Some differences in the toxicity profile were found between previous studies and this study (Table 5). The most noticeable characteristic of the toxicity profile in Korean patients was that nausea and vomiting were common. Korean patients might be more vulnerable to gastrointestinal complications of temozolomide than Western patients, though the exact mechanism could not be clarified. Thus, to mitigate gastrointestinal troubles anti-emetic prophylaxis should be considered for patients treated with temozolomide. However, Stupp et al. reported that fatigue (33.0%) was the most common event (2). The incidence of fatigue among patients with cancer is well documented, with 75%-99% of patients undergoing chemotherapy describing it as increasing with every cycle. Similarly, 69% of patients receiving radiation therapy reported increased fatigue with each treatment (12, 13, 14). It was also reported that the most common adverse event from radiotherapy was persistent fatigue and that approximately 60%-93% of cancer patients on radiotherapy experienced persistent fatigue (15, 16). Noticeably, Panet-Raymond et al. reported that fatigue (48.0%) and anemia (38.0%) were the most common toxicities of temozolomide (6), while Kesari et al. reported that leukopenia (47.7%) and neutropenia (34.1%) were the most common (8). These findings might be caused by the small number of patients included in the two studies.
No meaningful differences in toxicities with temozolomide by characteristics but by gender were found. It was reported that demographically females and patients under 50 yr old were more likely to experience nausea and vomiting after chemotherapy (17, 18, 19). However, we observed that only gender caused significant differences in vomiting: female experienced more than male. Also, it was observed that females experienced thrombocytopenia more than male, which is different in that thrombocytopenia is one of the most common toxicities after chemotherapy both to male and female (20, 21). Other characteristics did not appear significant.
Significant differences in toxicities with temozolomide between the two chemotherapy regimens were also found. More toxicities tended to occur in CCRT with temozolomide than adjuvant treatment. The rates of hematologic toxicities such as neutropenia, anemia and AST/ALT increases were higher in CCRT than in the adjuvant treatment. Moreover, non-hematologic toxicities, such as anorexia, alopecia, pruritus/itching, skin rash and lung infection, were also more common in the CCRT-treated patients. Although the exact reason for this phenomenon cannot be explained, chemotherapy plus radiotherapy is intuitively assumed to induce a greater number of toxicities than chemotherapy alone. In particular, alopecia and skin problems, such as pruritus/itching and rash, appear to be radiotherapy-induced toxicities. By contrast, headache and diarrhea were more common in the adjuvant period. Headaches may have been associated with the disease progression of malignant brain tumors.
Even though temozolomide toxicities might have some negative influences on patient quality of life, the intensive assessment of temozolomide toxicities is needed. Unfortunately, such studies have not been designed or performed. Most studies are simple and thus not sufficient to assess the overall toxicities of temozolomide. Understanding the toxicity profiles of temozolomide will result in nursing care customized to toxicities and levels. Additionally, more analyses and studies are required to determine if there is any relationship between adverse events and ethnic characteristics.
In this respect, our study has some limitations. The toxicity data may appear inadequate because we did not design this study prospectively. Moreover, we cannot exclude the side effects of radiotherapy, disease progression or the subjective complaints of the patients. For example, alopecia during CCRT could be caused by radiation or temozolomide, and neurological symptoms, such as headache and dizziness, could result from the tumor itself or temozolomide toxicity. Therefore, multi-centered, prospective studies are recommended to better assess patient quality of life and to reduce adverse effects, such as nausea and vomiting.
In oncology nursing, the awareness of evidence-based interventions for managing toxicities can be integral to the delivery of quality cancer care, and the information can be used to guide decision making in clinical practice. Familiarity with evidence on the management of toxicities will help nurses to identify and manage patients experiencing adverse events more proactively. Attention to adverse events, both hematologic and non-hematologic, is an important part of caring for glioma patients. Thus, it may be valuable to assess how toxicity management, such as dietary intervention, counseling, oral supplements, exercise and the use of anti-emetics, can affect the nutritional status of glioma patients and thus improve their quality of life, including the physical, emotional and social aspects.



 XML Download
XML Download