

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Inflammatory processes promote initiation and evolution of atheroma and contribute decisively to acute thrombotic complications of atheroma (1). White blood cell count is known to be an independent predictor of cardiovascular events and all-cause mortality (2). White blood cell subtypes, especially the neutrophil-to-lymphocyte ratio (NLR), has been proposed as a prognostic marker and seemed to be related to a proinflammatory state imposing worse clinical outcomes in patients with cardiovascular disease (3). Also NLR provides a simple and inexpensive method for assessment of inflammatory status in patients with acute coronary syndrome (4). Several studies have demonstrated a relation between the NLR and the severity of atherosclerosis and clinical outcome (5, 6, 7, 8, 9, 10, 11). However, the virtual histology-intravascular ultrasound (VH-IVUS) findings according to NLR were not well known.
Therefore, the aim of the present study was to evaluate the relation between NLR and plaque components assessed by VH-IVUS in patients with coronary artery disease (CAD).
MATERIALS AND METHODS
Patient population
This study was a retrospective, single-center study. From March 2006 to March 2010, a total of 399 CAD patients with 471 coronary lesions who underwent pre-intervention VH-IVUS at Chonnam National University Hospital were enrolled in this study. The presence of stable angina was determined by typical effort-induced chest pain which was relieved by resting. The presence of unstable angina was determined by chest pain within the preceding 72 hr with or without ST-T wave changes of positive cardiac biochemical markers. The presence of ST-segment elevation myocardial infarction was determined by >30 min of continuous chest pain, a new ST-segment elevation ≥2 mm on at least two contiguous electrocardiographic leads, and creatine kinase-myocardial band (MB) >3 times normal. The presence of non-ST-segment elevation myocardial infarction was diagnosed by chest pain and a positive cardiac biochemical marker without new ST-segment elevation. We excluded patients with subacute or late stent thrombosis, restenosis after stenting, coronary artery bypass graft failure, factors associated with increased risk of bleeding, severe heart failure or cardiogenic shock, important systemic disease, or creatinine ≥2.5 mg/dL, and patients in whom adequate IVUS images could not be obtained. The NLR was calculated as the ratio of neutrophil count to lymphocyte count. Based on the previously published article (11), we decided the cut-off value of NLR as 2.73, and we classified the patients into two groups according to the NLR on admission {low NLR group (NLR≤2.73 [370 lesions in 315 patients]) vs. high NLR group (NLR>2.73 [101 lesions in 84 patients])}.
Laboratory analysis
The blood samples were centrifuged, and serum was collected and stored at -70℃ until the assay was performed. Absolute creatine kinase-myocardial band levels were determined by radioimmunoassay (Dade Behring Inc., Miami, FL, USA). Cardiac-specific troponin I levels were measured by a paramagnetic particle, chemiluminescent immunoenzymatic assay (Beckman, Coulter Inc., Fullerton, CA, USA). Serum levels of total cholesterol, triglyceride, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol were measured by standard enzymatic methods. High-sensitivity C-reactive protein was analyzed turbidimetrically with sheep antibodies against human C-reactive protein; this has been validated against the Dade-Behring method (12).
Coronary angiographic analysis
Coronary angiogram was analyzed with validated QCA system (Phillips H5000 or Allura DCI program, Philips Medical Systems, Eindhoven, the Netherlands) (13). With the outer diameter of the contrast-filled catheter as the calibration standard, the minimal lumen diameter and reference diameter were measured in diastolic frames from orthogonal projections.
IVUS imaging and analysis
All IVUS examinations were performed a 20-MHz, 2.9F IVUS imaging catheter (Eagle Eye, Volcano Corp, Rancho Cordova, CA, USA) was advanced >10 mm beyond the lesion; and automated pullback was performed to a point >10 mm proximal to the lesion at a speed of 0.5 mm/sec.
Grey-scale IVUS and VH-IVUS data were analyzed by 2 independent observers. The levels of reproducibility for external elastic membrane, lumen, and plaque plus media cross-sectional areas using the Spearman rank-order correlation coefficients were 0.95, 0.97, and 0.97, respectively. Similarly, for plaque components by VH-IVUS, reproducibility for the fibrous, fibro-fatty, dense calcium, and necrotic core volume measurements using the Spearman rank-order correlation coefficients were 0.95, 0.92, 0.93, and 0.93, respectively.
Quantitative volumetric grey-scale and VH-IVUS analyses were performed across the entire lesion segment, and cross-sectional analysis was performed at the minimum lumen area sites and at the largest nectoric core sites. Conventional quantitative volumetric grey-scale IVUS analysis was performed according to the American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (14). Measurements were made by every 1-mm interval for the region of interest, which was defined as the segment between distal to proximal reference sites that were the most normal looking within 5 mm proximal and distal to the lesion. Volumetric data were generated by the software using Simpson's method. External elastic membrane and lumen cross-sectional areas were measured. Plaque plus media cross-sectional area was calculated as external elastic membrane minus lumen cross-sectional area; and plaque burden was calculated as plaque plus media divided by external elastic membrane minus lumen cross-sectional area. Total atheroma volume (TAV) was calculated by summation of atheroma area from each measured image as: TAV=Σ(external elastic membrane area-lumen area). The percent atheroma volume (PAV) was determined using the formula: PAV=100×(Σ[external elastic membrane area-lumen area]/Σ[external elastic membrane area]). VH-IVUS analysis classified the color-coded tissue into four major components: green (fibrous), yellow-green (fibro-fatty), white (dense calcium), and red (necrotic core) (15). VH-IVUS analysis was reported in absolute amounts and as a percentage of plaque area or volume. We defined thin-cap fibroatheroma (TCFA) as necrotic core ≥10% of plaque area in at least 3 consecutive frames without overlying fibrous tissue in the presence of ≥40% least 3 plaque burden (16).
Statistical analysis
The statistical Package for Social Sciences (SPSS) for Windows, version 19.0 (Chicago, IL, USA) was used for all analyses. Continuous variables were presented as the mean value±1SD; comparisons were conducted by Student's t-test, Discrete variables were presented as percentages and frequencies; comparisons were conducted by chi-square test, where appropriate. Multivariate analysis was performed to determine the independent predictor of TCFA. A P value<0.05 was considered statistically significant.
RESULTS
Baseline characteristics
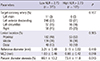
The baseline characteristics are summarized in Table 1. High NLR group had more acute coronary syndrome (ACS) compared with low NLR group. High NLR group had higher white blood cell counts and high-sensitivity C-reactive protein, and lower ejection fraction compared with low NLR group. The creatine kinase-myocardial band and troponin-I, and N-terminal pro-B type natriuretic peptide level were significantly higher in high NLR group.
Coronary angiographic findings
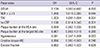
Coronary angiographic findings are summarized in Table 2. The minimal luminal diameter was significantly smaller and percent diameter stenosis was significantly greater in high NLR group.
Grey-scale and VH-IVUS findings
Grey-scale IVUS findings are summarized in Table 3. At the proximal reference, lumen cross-sectional area was significantly greater in high NLR group. At the minimum lumen area site, external elastic membrane cross-sectional area and plaque plus media cross-sectional area and plaque burden were significantly greater, and IVUS lesion was significantly longer in high NLR group. At the largest necrotic core site external elastic membrane cross-sectional area and plaque plus media cross-sectional area and plaque burden were significantly greater in high NLR group. By volumetric analysis, external elastic membrane volume and lumen volume and total atheroma volume were significantly greater in high NLR group.
VH-IVUS findings are summarized in figures. At the minimum lumen area site, absolute fibrous and necrotic core areas were significantly greater in high NLR group (Fig. 1A). At the largest necrotic core site, absolute and relative necrotic core areas were significantly greater in high NLR group (Fig. 2). By volumetric analysis, absolute fibrous and fibro-fatty and dense calcium and necrotic core volumes were significantly greater in high NLR group (Fig. 3A). Also TCFA was observed more frequently in high NLR group compared with low NLR group (Fig. 4).
We performed separate analysis in the stable angina and ACS patients. In a subgroup analysis, ACS patients had greater total atheroma volume and absolute necrotic core volume compared with stable angina patients (216.2±141.9 µL vs. 177.2±110.7 µL, P=0.004, and 26.9±23.2 µL vs. 20.0±15.8 µL, P<0.001, respectively), and TCFA was observed more frequently in ACS patients compared with stable angina patients (24% vs. 13%, P=0.009).
We performed analysis in patients with ACS and stable angina using reference value of NLR (NLR: 2.7), respectively. We classified the lesions into two groups according to the NLR on admission in patients with ACS {low NLR group (NLR<2.7 [n=242]) vs. high NLR group (NLR≥2.7 [n=92]) and stable angina {low NLR group (NLR<2.7 [n=126]) vs. high NLR group (NLR≥2.7 [n=11]), respectively}. In ACS patients, at the minimum lumen area site and at the largest necrotic core site, high NLR group had greater absolute nectoric core area compared with low NLR group (1.58±1.04 mm2 vs. 2.02±1.38 mm2, P=0.002, and 2.16±1.11 mm2 vs. 2.72±1.50 mm2, P<0.001, respectively), and high NLR group had greater total atheroma volume and absolute necrotic core volume compared with low NLR group (201.7±134.6 µL vs. 254.3±153.8 µL, P=0.002, and 24.3±20.8 µL vs. 33.7±27.7 µL, P=0.001, respectively), and TCFA was observed more frequently in high NLR group compared with low NLR group (35% vs. 20%, P=0.007). However, there were no significant differences in VH-IVUS parameters between high NLR group and low NLR group in stable angina patients using reference value (NLR: 2.7).
Independent predictors of TCFA
Independent predictors of TCFA are summarized in Table 4. The following variables were tested to determine the independent predictors of TCFA (variables with P<0.2 in univariate analysis): ST segment elevation myocardial infarction, NLR>2.73, total atheroma volume, high-sensitivity C-reactive protein, plaque burden at the minimum lumen area site, plaque burden at the largest necrotic core site, hypertension, creatine kinase-myocardial band, ejection fraction. ST segment elevation myocardial infarction (odds ratio [OR], 2.159; 95% CI, 1.000-4.660, P=0.050) and NLR>2.73 (OR, 1.848; 95% CI, 1.016-3.360, P=0.044) and total atheroma volume (OR, 1.003; 95% CI, 1.001-1.004, P=0.004) were independent predictors of TCFA.
DISCUSSION
The present VH-IVUS study demonstrated that 1) patients with high NLR had more acute coronary syndrome; 2) necrotic core components were significantly greater in high NLR group compared with low NLR group; 3) the TCFA was observed more frequently in high NLR group compared with low NLR group; and 4) ST segment elevation myocardial infarction, NLR>2.73 and total atheroma volume were independent predictors of TCFA.
Atherosclerosis is known to be an inflammatory process and NLR is associated with enhanced inflammatory response (17). Increased inflammatory response can cause atherosclerosis to destabilize and become clinical cardiovascular disease (18, 19, 20, 21). Muhmmed Suliman et al. (4) reported that high NLR increased mortality, thus providing an additional level of risk stratification in patients with acute coronary syndrome. In the present study, patients with high NLR had more incidence of acute coronary syndrome and had higher white blood cell counts and high-sensitivity C-reactive protein levels compared with those with low NLR.
Previous studies have reported that NLR was related to the development and progression of CAD (5, 22). In the present study, the percent diameter stenosis was significantly greater and total atheroma volume was significantly greater in patients with high NLR compared with those with low NLR. These results suggest that inflammatory process indicated by high NLR are associated with the progression of atherosclerosis.
Vulnerable plaque in coronary artery can progress to plaque rupture and thrombosis, and have a strong potential to induce ACS (23, 24). Also inflammation and necrotic core size play a greater role in the progression of atherosclerosis in diabetic subjects who experienced sudden coronary death (25). In the present study, the necrotic core component was greater and TCFA within culprit lesions was observed more frequently in patients with high NLR compared with those with low NLR. The results of the present study suggest that CAD patients with high NLR have a greater possibility having vulnerable plaque and higher inflammatory status, which can lead to acute coronary events. Therefore NLR can be used as a useful tool to detect not only significant atherosclerosis but also plaque vulnerability in patients with CAD.
There are several limitations to be mentioned. First, the present study is retrospective single center study, so is subject to limitations inherent in this type of clinical investigation. Second, IVUS and VH-IVUS imaging were performed at the discretion of the individual operators leading to potential selection bias. Third, there is limitation using 20 MHz IVUS because this low frequency IVUS has a limitation to detect the plaque in detail, especially in the near field. Fourth, heavily calcified plaques may induce an artifact regarding the codification of plaques by VH-IVUS resulting in an increase in necrotic core content. Fifth, serial follow-up of serum neutrophil and lymphocyte levels were not performed. Therefore, we did not demonstrate the impact of sequential change of NLR levels on plaque components.
In conclusion, the present study demonstrates that CAD patients with high NLR had more vulnerable plaque components (greater necrotic core containing plaques) than those with low NLR. Our results of the present study suggest that CAD patients with high NLR have a greater possibility having vulnerable plaque and higher inflammatory status, which can lead to acute coronary events. Therefore NLR can be used as a useful tool to detect not only significant atherosclerosis but also plaque vulnerability in patients with CAD.






 XML Download
XML Download