

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Congenital myotonic dystrophy (CMD) is an autosomal dominant neuromuscular disorder with major features including muscular hypotonia, respiratory failure, feeding problems, developmental delay, and less commonly systemic involvement including congenital cataract, thyroid dysfunction, and abnormal cardiac manifestation (1, 2). Cardiac involvement displays the following: conduction system disturbances, atrial and ventricular arrhythmias, hypertrophic cardiomyopathy, and sudden cardiac death (2, 3, 4). In patients with CMD, conduction disturbances including atrioventricular (AV) block generally occur during adulthood (5). There has been no recorded report of complete AV block in a neonate with CMD. We present a case of transient complete AV block completely managed with temporary transcutaneous pacing in a preterm neonate with CMD.
CASE DESCRIPTION
A 1,630 g female baby was born at 31+4 weeks of gestation by emergency Cesarean section to a spontaneously pregnant, nulli, non-aborted, 33-yr-old mother due to persistent bradycardia of the fetal heart rate of 50 beats/min (bpm) on 11 December 2011. On pregnancy history, polyhydramnios (amniotic fluid index was 35) had been noted at 30+6 weeks of gestation at a local clinic. The result of amniocentesis for the fetal karyotype was normal. A decrease in fetal movements was detected from 31+3 weeks of gestation. At birth, the baby's Apgar score was 2 at 1 min, and she showed no respiration and movement, with a heart rate of 50-60 bpm. She was treated with ventilator assistance. At that time, the vital signs were as blood pressure (BP) of 57/34 (mean 41) mmHg, heart rate of 60 bpm, and O2 saturation (SpO2) of 50%. The initial venous blood gas analysis showed a pH of 7.099, pCO2 of 88.4 mmHg, and HCO3- of 27.4 mM. Despite administration of 100% oxygen, SpO2 was 60% and the heart rate was 60 bpm. As a result, cardiopulmonary resuscitation with intravenous epinephrine was performed. However, bradycardia of 60 bpm was persistent. A chest X-ray revealed respiratory distress syndrome with cardiomegaly (cardiothoracic ratio 0.6), thin ribs, peripheral thinning, and floating clavicles (Fig. 1A). Surfactant was administered intratracheally. At 1 hr after birth, BP was decreased to 42/19 (mean 29) mmHg. Continuous intravenous infusion of dopamine, dobutamine, and epinephrine was started.
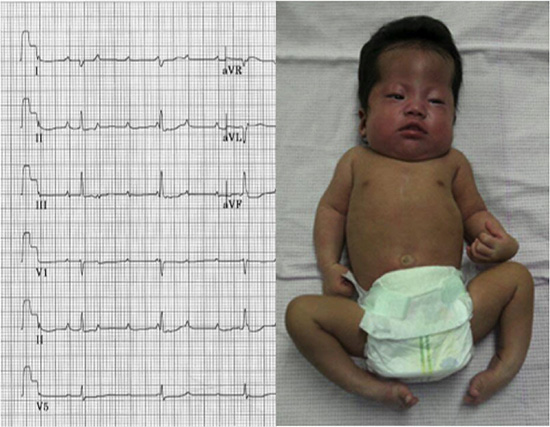
Electrocardiography (ECG) showed a complete AV block with an atrial rate of 150 bpm and a ventricular rate of 54 bpm (Fig. 2A). Echocardiography showed normal ventricular function with patent ductus arteriosus (PDA). For the treatment of the complete AV block, atropine and isoproterenol were administered, but there was no improvement. We applied temporary transcutaneous pacing (Responder 2000, Cardiac Science Corporation, USA) under sedation with midazolam at 4 hr after birth (Fig. 1B). The BP increased to 51/37 (mean 44) mmHg and the SpO2 gradually increased up to 100% on FiO2 of 0.21. Thirty two hours after transcutaneous pacing, the ECG completely recovered to a normal sinus rhythm of 135 bpm (Fig. 2B). The temporary transcutaneous pacing was removed at that time. However, there was a 3×1 cm-sized third degree contact burn, and escharotomy was done by a plastic surgeon at the removal site of the pacing at the apex (Fig. 3A). The burn wound healed by one month after birth.
Blood analysis revealed CK-MB of 15.6 U/L, troponin-I of 0.01 ng/mL, and N-terminal pro b-type natriuretic peptide of 5,575 pg/mL. In the serum autoimmune test of the mother, antinuclear antibody (ANA) and lupus anticoagulant were negative. Likewise, in the patient's test, ANA, anti-Ro/SSA, and anti-Ra/SSB antibodies were negative.
On physical examination, the baby showed typical features of CMD, such as frontal bossing, weak facial expression with tented upper lip, high arched palate, generalized hypotonia with hyporeflexia, and bilateral talipes equinovarus (Fig. 3B). Genetic study for CMD revealed a congenital form of more than 1,000 copies of cytosine-thiamine-guanine (CTG) trinucleotide repeat at the 3' untranslated end in the myotonic dystrophy protein kinase gene (DMPK) on chromosome 19 (Fig. 4A). According to the genetic study of the parents, the father was normal and the mother showed 150 copies of the CTG repeat, which was compatible with CMD carrier status (Fig. 4B).
For nutrition, gavage feeding was started at 9 days of birth. Additional parenteral nutrition was given for 2 months due to the persistence of the respiratory difficulties, weak sucking, and swallowing difficulties. On the 88th day after birth, she began to be fed orally. She was successfully weaned from the ventilator at 115 days of birth despite poor respiratory effort and copious secretions. At 137 days of birth, she was discharged from the hospital (Fig. 3C). Currently, she is 16 months old in corrected age and has a weak facial expression, along with developmental and growth delays. She exhibits head control, but cannot roll over or sit unaided. However, there are no respiratory difficulties and arrhythmia has not recurred.
DISCUSSION
CMD is a multisystem disorder characterized by neonatal hypotonia, joint contractures, facial diplegia, fatal respiratory failure, feeding problems, cardiac conduction abnormalities, and developmental delay (1, 6). It presents at birth or during the first year after birth (1, 2). In the neonatal period, mortality is high with a rate of 17% to 41%. A common cause of death is respiratory insufficiency (6). Prenatally, reduced fetal movements or polyhydramnios that reflect intrauterine hypotonia may induce concerns of CMD (7). The genetic mechanism is understood to be caused by expansion of the CTG repeat in the 3' untranslated region of the DMPK gene on chromosome 19 (8, 9, 10). There are possible correlations between the presence and proceeding of ECG abnormalities, the timing of cardiac complications, and the risk of major cardiac events and the number of CTG repeats (1). The pathology of cardiac involvement is known as interstitial fibrosis, hypertrophy of myocardiocytes, fatty infiltration, and focal myocarditis (11). Cardiac evaluation consisting of a basal ECG, echocardiogram, and Holter monitoring should routinely be done in all patients with CMD (1, 2).
Conduction system abnormalities are the major cardiac abnormalities observed in CMD (1, 5). A recent study (12) reported the prevalence of conduction abnormality in patients with myotonic dystrophy including CMD between 1980 and 2010. The prevalence of conduction abnormalities were grade 1 AV block of 28.2%, grade 2 AV block of 2.1%, frequent premature ventricular contractions of 14.6%, right/left bundle branch block of 4.4/5.7%, atrial fibrillation or flutter of 5%, and non-sustained ventricular tachycardia of 4.1%. The prevalence of a complete AV block was rare (0.3%), and did not occur in the neonatal period. Another study (5) reported the prevalence of ECG abnormalities in seven young patients with CMD. The prevalence were grade 1 AV block of 5 (71.4%), left anterior fascicular block of 3 (42.8%), left bundle branch block of 1 (14.3%), and left posterior fascicular block of 1 (14.3%). To the best of our knowledge, a complete AV block accompanied by CMD during the neonatal period, as in our case, has not hitherto been reported (13).
A congenital complete AV block may occur due to maternal autoimmune diseases (14). In our case, there was no clinical or laboratory evidence of maternal or fetal autoimmune disease. The 2008 guidelines of the American Heart Association, the American College of Cardiology Foundation, and the Heart Rhythm Society recommend that a permanent pacemaker be implanted in patients with congenital complete AV block with no delay (15). However, there are several problems with doing this in neonates and young infants. They are very small and grow quickly, so the position of the pacemaker leads or generator can change (16). Temporary transcutaneous pacing has been used broadly in older children and adults to manage acute bradycardia. The main advantage of this technique is that it is non-invasive and relatively simple to use (17). However, in a preterm neonate with complete AV block, transcutaneous pacing has a relatively large size of the external pacing electrodes and the risk of burn where the pacing electrodes have not been well insulated (17). To prevent the burn, it is necessary to observe electrode contact sites and to use the lowest effective current (17). Although there was a burn injury on the chest in our case, the temporary transcutaneous pacing was removed after 32 hr without any major problems.
In conclusion, when a newborn has a complete AV block, the physician should consider the possibility of the CMD and conduct a careful physical examination.




 XML Download
XML Download