

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Familial disease refers to the increased risk of disease experienced by relatives of patients (1). Familial disease is an epidemiologic concept where members of a family share genetic and environmental factors. Prediction of familial risk profiles relies on the presence of susceptibility genes, early age at onset or a family member with the same disease (1). The familial risk assessment provides a practical risk management plan for certain diseases based on the family history (2). For example, familial breast cancer is characterized by several features such as male involvement, bilateral or recurrent breast cancer at the same side and familial history of breast cancer or ovarian cancer and the BRCA gene mutation. By thorough inspection of the familial degree, prophylactic mastectomy or oophorectomy may be recommended, which may reduce the breast cancer risk significantly if there is a strong family history (3, 4).
Aggregation of ankylosing spondylitis (AS) or clustered incidence in the family has been reported previously. The recurrence risk was high in familial cohorts than sporadic cohorts or the general population (0.2%-0.9%), and was generally higher in first degree family members (5.9%-15%) than relatives with other degrees, and higher in monozygotic twins than dizygotic twins (5, 6). About 10%-40% of AS patients were reported to be familial in the literature (7, 8, 9).
Phenotype studies on familial AS, comparing it with sporadic form of AS or spondyloarthropathy, have been published. These studies reported not only increased incidence of AS in the familial cohort but also the distinct features of the disease. Said-Nahal et al. (10) reported that familial spondyloarthropathy showed clustering of arthritis and uveitis. Subjective outcomes such as pain, disability and objective radiographic changes were influenced by familiality (10). A UK study reported that familial AS was a milder disease than the sporadic disease in terms of spinal mobility, physical, emotional and social well-being (11). According to a Spainish study, being female and having a young age at symptom onset, longer disease duration, uveitis, HLA-B27, higher pain visual analogue scale (VAS), higher Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and a good response to non-steroidal anti-inflammatory drugs (NSAIDs) were reported to be associated with familiality (12). However, there are some discrepancies between the studies in the characteristics associated with familiality and severity, and the treatment response and disease course have not been explored in association with familiality in some of these studies.
Familial history is one of the conditions of spondyloarthropathy to the extent that it is included in the classification criteria of spondyloarthropathy (13). The contributions of HLA-B27 and familial aggregation in AS have been regarded as evidence of the genetic influence in that disease (14). An enormous paper about the HLA-B27 gene being the most important genetic factor in the susceptibility of AS has been published (7, 8). The high risk of AS in HLA-B27 positive first degree relatives has been reported previously (9). However, the presence of HLA-B27 cannot discriminate between familial disease and sporadic disease since HLA-B27 is present in as many as 90%-100% of AS patients. Furthermore, HLA-B27 negative familial AS has also been reported (10). Therefore, it is worthwhile to identify the shared features other than HLA-B27 that occur in the familial forms of AS.
The aim of this study was to explore the incidence of familial AS in Korea, and to compare the phenotype of the disease between the familial disease and sporadic disease.
MATERIALS AND METHODS
Study population
AS patients in the outpatient clinic of the Seoul National University Hospital were consecutively enrolled from June 2012 to December 2012. Out of a total of 215 patients investigated, 11 patients who did not meet the 1984 modified New York criteria were excluded (15).
Index patients had a face-to-face interview with well-trained researchers to elicit their familial pedigree tree. For more information, telephone interviews were conducted with a member of the family as to whether he/she was a candidate for AS. If necessary, the candidates were invited to the clinic for evaluation and confirmation of AS. Demographic data including age, sex, body weight, height, smoking, familial history, current or prior clinical features (advanced features in radiography, psoriasis, inflammatory bowel disease, arthritis, enthesitis and uveitis), presence of HLA-B27, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and treatment used were obtained by questionnaire surveys and a retrospective review of the medical report.
Definition of familiality
AS patients with a positive one or more first to third degree relatives with AS, defined by the 1984 modified New York criteria, were classified as having familial AS. Familial pedigrees were drawn for the first to third degree family members including the parents, children, siblings, grandparents, grandchildren, nephew, aunts, uncles and cousins. Patients were considered to have sporadic AS when they denied having relatives with AS.
Statistical analysis
Recurrence risks were defined as the ratio of the number of AS family patients/familial members in relatives of affected AS subjects. Demographic and clinical characteristics of the study sample are described separately for familial AS patients and sporadic AS patients and according to gender and disease duration among familial AS patients. Characteristics of familial AS compared to sporadic AS were analyzed using chi-square tests or Fisher's exact tests to compare categorical variables and Student's t-test or Mann-Whitney test to compare continuous variables, as appropriate. All statistical analyses were performed with SPSS 19.0 for Windows (SPSS 19.0 Inc., IBM Company, Chicago, IL, USA).
RESULTS
Characteristics of the study population
A total of 204 AS patients (165 males and 39 females, mean age 37.0±13.1 yr, mean disease duration 10.8±7.7 months) were evaluated. Percentage of patients who were positive for HLA-B27 was 85.8%. Thirty-eight (18.6%) of 204 proband AS patients had a familial history. Of 2,412 family members investigated, 50 (33 males and 17 females) familial patients were identified.
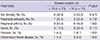
Recurrence risk of AS
Recurrence risk in all AS patients for first, second, and third familial degrees was 3.0%, 1.7%, and 1.5%. When restricted to the familial AS group, the recurrence risks increased to 14.6%, 5.2%, and 4.4%. If the relationship was close to the proband, the risks were higher in a dose dependent manner. In first degree families, siblings rather than the parents or children were more prone to have familiality (Fig. 1).
Characteristics of the familial AS compared to sporadic AS
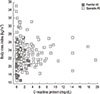
Significantly lower ESR and CRP were observed in familial AS patients compared to their sporadic AS counterparts (ESR, 22.6±22.2 vs 35.4±34.4, P=0.029; CRP, 1.24±1.7 vs 2.43±3.3, P=0.003) (Table 1). A significantly lower body mass index (BMI) was noticed in the familial group (21.9±2.7 vs 23.7±3.3, P=0.002). Familial AS was distributed in the quadrant of low CRP/low BMI (Fig. 2). HLA-B27 positivity was significantly higher in familial AS (97.4% vs 83.1%, P=0.044). Axial symptoms and the presence of sacroiliitis proven by plain radiography and advanced radiographic findings such as syndesmophytes or sacroiliac ankylosis were not different between the two groups. Assessment of the pattern of arthritis revealed that oligoarthritis was significantly less common in the familial group, which also had less asymmetry. Particular parts of any joint disease were not different (data not shown). Peripheral enthesitis including dactylitis, Achilles tendinitis and plantar fasciitis were less commonly observed in familial AS. Extraarticular manifestations including psoriasis, uveitis and inflammatory bowel disease were not affected by familiality.
Familial AS patients according to age, sex and disease duration
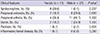
There was no difference by sex in familial patients (Table 2). The formation of syndesmophytes was more seen in female patients, statistically not significant, though. Earlier disease onset is regarded as a feature of familial disease in various diseases such as familial breast cancer and familial colon polyposis. Therefore, we investigated the age at onset of the disease and divided the familial AS patients by short (<10 yr) or long disease (≥10 yr) duration to explore the differences (Table 3).
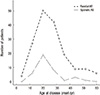
Age of disease onset seemed to be earlier and the percentage of female patients was lower in the familial AS group; however, both these findings did not reach statistical significance (Table 1). In the graph directly comparing age at disease onset (Fig. 3), the two groups showed no differences and demonstrated the same peak of development in the 20s. In the familial AS patients, disease duration was not a factor that showed any difference between the short and long duration of the AS groups. However, higher female involvement and more peripheral arthritis were observed in the early AS with a disease duration of less than 10 yr group, whereas more peripheral arthritis and more uveitis were present in established AS with a disease duration of more than 10 yr, but these differences did not reach statistical significance.
DISCUSSION
The current report describes the increased occurrence of AS within families. The different phenotypes of familial AS compared to sporadic AS were explored. Lower inflammatory conditions in spite of the higher prevalence of HLA-B27 in the familial AS group were remarkable in this report. This is similar to the findings from a study that showed that familial disease was milder in metrological measures than sporadic disease (11). To the best of our knowledge, this study is the first to examine familial AS and its clinical manifestations in Asia.
Familial studies have been published primarily in Europe (10, 11, 12, 16, 17). Although higher familial recurrence has consistently been recognized, discrepancies have been found among the studies. Calin et al. (11) found that there were milder conditions in familial AS as assessed by spinal mobility, physical social and pain score. In contrast, Paardt et al. (16) did not find difference in phenotype expression. In a study from Spain, familial AS patients had a poorer pain visual activity score compared to sporadic AS patients. Young age at symptom onset and female dominance, higher frequency of uveitis, and HLA-B27 prevalence and a better response to NSAIDs in familial AS have also been addressed (12). In the Belgian study, psoriasis and uveitis were significantly higher (17). Dissimilarly, clustering of arthritis and uveitis in familial disease were observed and no relationships between familiality and psoriasis and inflammatory bowel disease were found in a report from France (10). However, the definition of familiality and the extent of proband patients were different among the studies. We enrolled Korean AS patients and familial AS patients who were both defined by the 1984 modified New York Criteria for AS (15).
Strikingly, acute phase reactants, generally responsible for disease activity in AS, were lower in familial patients than sporadic AS patients. It is a finding that supports that of previous report of Calin et al., in which familial AS was found to be a milder disease than sporadic disease in terms of spinal mobility, and physical, emotional and social well-being. One study from Spain reported that ESR and CRP were not different at the time of study (11), although, these cannot reflect genuine activity of the disease or predict the disease phenotype without the concomitant treatment such as TNF inhibitor or DMARDs being adjusted. Our study reported the ESR and CRP at diagnosis and found lower inflammatory conditions in familial AS than in sporadic disease. One study reported that the disease severity as assessed by BASDAI and BASFI was demonstrated to be correlated with familiality, leading one to consider that the severity of the disease is genetically determined (18). At-risk families may have had a susceptibility gene rather than a severity gene (11). However, evaluation of disease burden and activity requires more than serum ESR and CRP, these data should be interpreted with caution.
Lower BMI in the familial group was observed. Obesity is a condition in which inflammatory cytokines are increased (19). This suggests that lower inflammatory conditions along with lower ESR and CRP in familial AS are noticeable features. The response to infliximab in AS was poorer in obese patients (20) although this cannot entirely explain the outcomes of familial AS. Therefore, it would be worthwhile to evaluate the treatment response according to BMI in the familial disease in the future.
In our study, early disease onset or diagnostic delay were not observed to be associated with familial AS. This differs from a previous report, in which the relatives of probands who were younger had a higher risk of having AS (11, 21). Recognition of the AS history in family members may raise alertness to the symptoms of spondyloarthropathy and may encourage earlier inspection for the presence of HLA-B27 or the development of the disease. However, Korean families of AS sufferers did not show any difference in the age of symptom onset or the diagnostic time-point. Similarly, age of onset was not a phenotype of familiality in the French study (10), suggesting that the age of disease onset is primarily determined by nongenetic causes (18). Furthermore, radiographic advancity in the axial or sacroiliac joint was not different between familial AS and sporadic AS, probably because the disease duration was not different in both groups.
The sex ratio in our patients was not different between familial and sporadic AS (28.9% vs 16.9%, P=0.139). However, there was a trend for female predominance. A larger cohort may show a difference between the two groups in the sex ratio in the future study. In the recent report from Spain, female patients were predominant in the familial cohort (12). In contrast, a Belgian study reported the same sex prevalence (17). The importance of female sex in the familial disease has been previously described, with the young female index case having a higher familial recurrence among children and siblings (22). Generally, females are thought to be more resistant to getting spondyloarthritis than male. Therefore, an interpretation was given that female sex within a family cohort contributes to susceptibility rather than severity by females more easily passing the disease to their offsprings than males (23). However, research on the X chromosome failed to show any genetic evidence for susceptibility (24), and other genes responsible for susceptibility are still to be elucidated.
Regarding the differences between the sexes in familial AS, female patients from a French familial cohort showed significantly less radiographic sacroiliitis than male patients, although they had a similar incidence of symptomatic buttock pain (10). In addition, the longer the disease duration, the higher the male/female ratio in the French cohort (10). This is a supportive evidence that the female factor is important for predicting susceptibility to the disease rather than severity (22). Our familial patients did not show a difference between the sexes, possibly due to the small numbers of the patients.
A familial risk model study revealed that heritability depends on genetic factors rather than environmental factor, and if the genetic factors are implicated, fewer than 5 genes are involved (5, 18). However, the GWAS study did not find any difference between the familial group and sporadic group (25). Although a significantly higher prevalence of HLA-B27 was demonstrated in familial AS patients in this study, the presence of HLA-B27 still cannot predict or discriminate familial disease in the AS cohort. However, we witnessed again the high recurrence of AS in the familial group in this Korean patients as in the European patients, and the closer the relationships, the higher the recurrence risk, indicating higher susceptibility in the familial group. Clustering of certain phenotypes (e.g. arthritis and uveitis) in the familial AS group, suggesting a specific genetic or environmental factor contribution to specific phenotypes, has been reported. The current study suggests that further studies of the genetic determinations of such phenotypes are indicated, and that understanding the familial disease by phenotypes may further expand knowledge about the pathophysiology of AS. Practically, this study also indicates that identification of the familial history may bring a distinct approach to patients with AS and prognosis of the disease.
The questionnaire or telephone inquiry based acquisition of information regarding the familial history in the study may have caused errors in data sourcing. Therefore, potential familial disease patients could have been misclassified into sporadic disease or vice versa. To avoid error, we enrolled consecutive outpatient patients and performed investigations pertinaciously.
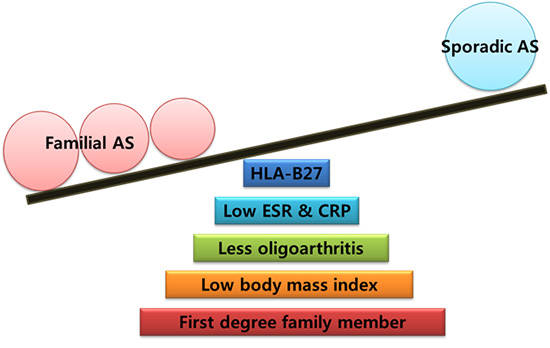
In conclusion, we report that Korean AS patients with a familial history have a higher presence of HLA-B27 than sporadic AS. The recurrence risk in the familial AS is highest in the first degree relatives, indicating higher susceptibility to the disease. Distinct phenotypes of familial AS are lower frequency of oligoarthritis, lower ESR and CRP at diagnosis and lower body mass index.


 XML Download
XML Download