

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Knowledge translation strategies for evidence-based clinical decision-making are embodied in Clinical practice guidelines (CPGs). In Korea, more than 100 CPGs have been developed in the last decade, and the types and development of CPGs are increasing (1, 2, 3). Nevertheless, there have been no discussions on the scientific methodology of guideline development or an appraisal for the developed CPGs. Moreover, the quality management of CPGs such as accreditation by prestigious institutions differs according to the organization developing the CPGs.
The purpose of an appraisal was to enhance the quality of information that CPGs provide to decision-makers and recommendations that have been developed using critically evaluated high-quality processes (4). For this purpose, in Europe and North America, where CPGs are actively applied, quality management of CPGs is performed using standardized tools or outlining the requirements developers must follow during the development process (5). In Korea, the Korean Academy of Medical Sciences (KAMS), the federation of professional societies of medical sciences in Korea, established a center for appraisal of clinical practice guideline in 2013 and took a major role in quality management of CPGs through the peer assessment by using the Appraisal of Guidelines for Research & Evaluation (AGREE) instrument.
AGREE instrument is a tool that assesses the methodological rigor and transparency by which a CPG is developed (6). The original AGREE instrument was developed in 2003 in collaboration with researchers from 13 countries. In 2009, AGREE II was produced, improving the reliability, validity, and performance of appraisal. In Korea, a translation of the original AGREE instrument was introduced in 2006. In 2010, AGREE II was translated into Korean and distributed to Korean medical societies. The usefulness of AGREE II have been verified through various quality assessment studies of specific diseases (8, 9, 10, 11), international comparison of the level of guideline development (12, 13), and overall quality assessment of CPGs developed in specific countries (14, 15, 16, 17).
However, differences in the developmental environments, health care systems, and medical cultures across the countries make it difficult to apply AGREE II uniformly to all assessments. Consequently, AGREE II is simply a comprehensive reference, not any details of the proposed standards (7). In addition, Korean medical societies did not have enough experience developing CPGs and applying AGREE II. These limitations have led to obstacles appraising CPGs, including a lack of consensus among appraisers and a significant score variability. That is, there is an inter-rater disagreement.
Therefore, the Korean AGREE II Scoring Guide (hereafter, Scoring Guide) was developed to reduce these inter-rater differences (7). By reflecting the characteristics of the developmental environment of Korea, it provides detailed evaluation criteria for each item. It is expected to reduce the variation in scores among appraisers and presents a desirable target level for the development of CPGs.
This study examined the effects of the Scoring Guide, with an emphasis on reducing inter-rater differences and improving assessment reliability.
MATERIALS AND METHODS
AGREE II
AGREE II consists of 23 key items organized within six domains followed by two global rating items ("Overall assessment"). Each item is rated on a 7-point scale (1 = strongly disagree to 7 = strongly agree). Each domain captures a unique dimension of guideline quality. AGREE II recommends that each guideline be assessed by at least two appraisers, and preferably four, to increase the reliability of the assessment.
Scoring guide
The Scoring Guide was developed in accordance with Korean AGREE II. The first draft established requirements for anchor points 1, 3, 5, and 7 for each of the Korean AGREE II items and presented a specific checklist for each anchor point. Final agreement was derived through a modified Delphi consensus process. Thirteen specialists participated in the process and the modified Delphi was conducted twice.
Assessment and appraisal
Appraisers were randomly assigned to two groups (Scoring Guide group and Non-Scoring Guide group). The Korean AGREE II instrument was provided to both groups. However, the scoring guide was offered to Scoring Guide group only. Total 14 appraisers were participated and each guideline was assessed by 8 appraisers.
Clinical practice guidelines
Two CPGs that were officially submitted for appraisal to the Korean medical guideline information center (KoMGI) were appraised (Table 1). The KoMGI recognizes Korean AGREE II as the only official tool for appraisal, but the Scoring Guide was applied for this study with the consent of the developers.
Statistical analysis
A descriptive analysis of the distribution of domain scores according to the group was performed. To evaluate the reliability of the Korean AGREE II Scoring Guide, domain-specific intra-class correlations (ICCs) were calculated. The consistency of scores among appraisers was assessed by analyzing the correlation between the scores within the group. The statistical program SPSS for Windows 18.0 (SPSS, Chicago, IL, USA) was used. P values of 0.05 or less were considered significant.
RESULTS
Distribution of scores
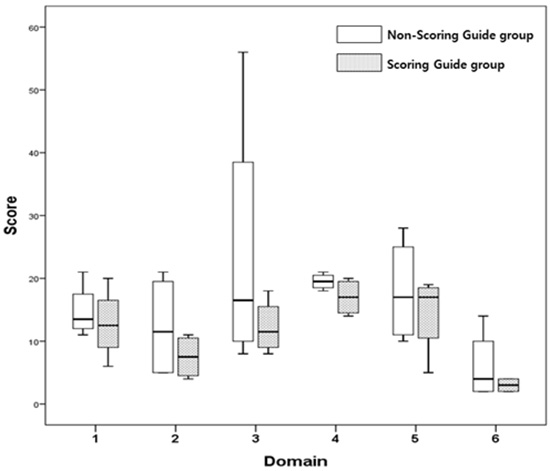
Compared to the Non-Scoring Guide group, the distributions of the domain-specific scores in Scoring Guide group were characterized by low scores and low deviation for both CPGs. The differences were notable for domain 2 (Stakeholder involvement), domain 3 (Rigor of development), and domain 5 (Applicability) (Fig. 1). However, the difference was not statistically significant.
Reliability
Inter-rater reliability was analyzed by comparing the ICCs between the groups. The Scoring Guide groups had higher ICCs for both CPGs and this was common in all domains, except domain 4 (Clarity of presentation) and domain 6 (Editorial independence). Domain 3 and domain 5 were particularly significant. The overall scores were significantly higher in the Scoring Guide groups for both CPGs (Tables 2, 3).
DISCUSSION
Although quality management policy regarding CPG development varies widely across the countries, a strict quality assessment based on the AGREE II instrument is a common feature. This means that a thorough understanding and proper applications of AGREE II are essential for quality management of CPGs. In Korea, AGREE II was translated and distributed to medical societies in 2011. Nevertheless, inter-rater disagreement issues still exist. So, the Scoring Guide was developed to reduce inter-rater differences. This study examined the effects of the Scoring Guide on the reduction of inter-rater differences.
Most scores for the two groups were comparable, and the Scoring Guide groups showed higher reliability for both CPGs. They showed a stronger correlation among appraisers and higher ICC values for most domains, especially domain 2 (Stakeholder involvement), domain 3 (Rigor of development), and domain 5 (Applicability).
To better understand the results, the characteristics of the appraisers' environment, which affect their decisions, must be considered (11, 18, 19, 20). In the Korean healthcare environment, stakeholder involvement is an unfamiliar concept. Participation of the patients and citizen is seldom guaranteed, and even if they participated, their power and rights are generally weak (21, 22). As a result, only experts are recognized as stakeholders. This lack of stakeholder involvement experience in health policy and various definitions of stakeholder among appraisers are thought to have influenced the results. In this study, we found that the Scoring Guide reduced the gap in experience and understanding among appraisers by providing clear standards regarding the stakeholder and level of participation.
Another distinct domain is applicability. Applicability evaluates whether facilitators and barriers to its implementation and the potential resource implications of applying the recommendations have been considered. Strategies used to promote the implementation of CPGs are diverse, and the effect of application differs depending on the user's environment (23, 24, 25). Since there are few or no implementation strategies or efforts to promote the implementation level in Korea, differences in awareness and environments across appraisers are thought to affect inter-rater differences. In this respect, the Scoring Guide that provides specific criteria related to resources and methodology for measuring the level of implementation could complement the gaps in experience and awareness among appraisers.
This study suggests that the low reliability across appraisers arises from the effects of the healthcare environment and characteristics of the appraisers, rather than the validity of the Korean AGREE II instrument itself. Using these findings, we can find ways to overcome those limitations, and expand the use of evidence-based CPGs in Korea.
Low reliability was noticeable for low-quality CPG development. This means that enhancing CPG developmental competency is the first step in CPG quality management, to improve the reliability of appraisers. Therefore, priority should be placed on the development of high-quality CPGs, and developers should be provided with tools and programs for developing CPGs. Two guidebooks related to de novo and adaptation methods have been developed and disseminated, but few societies are aware of these manuals and active implementation strategies are insufficient (26). Guidebooks and programs to aid guideline development using scientific methodology and covering comprehensive developmental processes could be an effective strategy.




 XML Download
XML Download