

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rewarding effect of alcohol is mediated partly via release of endogenous opioid peptides (1). The central opioid activity is increased after alcohol consumption (2). It was reported that the level of β-endorphin in plasma and hypothalamus increased after acute and chronic administration of alcohol to mice (3). It is thought that the opioid system, which is activated by alcohol administration and acts on the brain's reward pathway, results in increasing and maintaining drinking behavior (4). On this account, when the opioid system activation is blocked by a nonspecific opioid receptor antagonist such as naltrexone, the pleasurable effects created by alcohol administration are blocked, which would result in the suppression of alcohol intake (5).
Many studies have proved the effectiveness of naltrexone in treating alcoholism. It reduces relapsing to heavy drinking and alcohol consumption (6, 7, 8). However, its efficacy is seemed to be different according to the clinical variables. Several studies identified some clinical variables associated with a positive response to naltrexone: earlier onset age, positive familial loading of alcoholism, higher alcohol craving, and sweet taste preference phenotype (9). Laaksonen et al. (10) reported that preference for sweets had a strong correlation with treatment outcome with naltrexone and sweet preference might be used as a predictor for better treatment results in alcoholics. The sweet taste preference may act as a putative probe of brain opioid function and predict variations in response to naltrexone treatment (11).
Besides the sweet taste preference, a few studies suggested that spicy food preference was associated with the opioid system and alcohol drinking (12, 13, 14). Capsaicin is a main component of the spicy flavor of red peppers. Capsaicin administration resulted in increase of proopioimelanocortin (POMC) mRNA in the arcuate nucleus of Sprague-Dawley rats (13). In addition, it was reported that β-endorphin in cerebrospinal fluid in the cerebellum and medullar oblongata of white mice increased after 30 min when injected with capsaicin intrathecally (15). In addition to capsaicin's association with the opioid system, its administration affects alcohol intake. After intraperitoneal administration of capsaicin in C57BL/6 mice, alcohol intake was suppressed from 2 hr to 2 days after capsaicin administration (12). In our preliminary study, there was a tendency of more suppression of acute alcohol's effects by naltrexone in spicy food preferring social drinker (14). These results imply that capsaicin administration may increases the central opioid activity. In spite of the fact that eating spicy food is painful, some people still prefer spicy food.
On this point, we presumed that central opioid system is activated more in those who prefer spicy food than in those who do not prefer it, although it is not certain so far that its activation is related to increased affinity or increased number of central opioid receptors. We hypothesized that, with alcohol administration, the acute alcohol's effects related to activating the central opioid system are more remarkable in those who prefer spicy food. Also, acute alcohol's effects related to activating the central opioid system are blocked more remarkably by the administration of naltrexone in those who prefer spicy food. The aim of the present study is to investigate the differences in subjective acute response to alcohol and naltrexone's effects on them among social drinkers who prefer spicy food to various degrees.
MATERIALS AND METHODS
Subjects
Subjects of this study were 30 men who did not meet alcohol dependence requirements. We excluded subjects who experience facial flushing when drinking alcohol because they were likely to complain of physical discomfort when drinking the amount of alcohol required for this study. Also, four subjects were excluded during statistical analysis, as they did not participate in the eighth and ninth day or did not answer all the questions on the measuring instruments. Therefore, a total of 26 subjects were included in the statistical analysis.
Food preference scale (FPS)
To investigate food preferences, we developed FPS. First, fifteen medical students freely wrote out their choices of the representative food of each taste category (spicy, bitter, sweet, sour, salty). Then, five representative foods of each taste were chosen according to their frequency. After the respondents placed them in the order of representation of each taste again, we decided three representative foods of each taste in accordance with their ranking. These fifteen different foods were then randomly presented.
The preference for each food was measured by a visual analogue scale (VAS). Respondents checked the grade of preference on the 100 mm horizontal line that contained the phrases "don't like it" at the left end, and "like it very much" at the right end. We decided the preference of each food by taking measurements from the left end of the VAS to the indicated point in units of millimeters. That represented the preference for each food. Spicy food preferences were presented by discerning the average preference of three kinds of spicy food (panbroiled octopus with hot pepper paste, rice-cake with hot pepper paste, and stichy noodles with hot pepper paste).
Biphasic alcohol effects scale (BAES)
BAES consists of 12 items that measure the stimulative effects of alcohol, i.e., unsettled, energetic, being at ease, being excited, uplifted, dizzy, clearheaded, sentimental, inspired, talkative, active and having stamina. And it consists of 12 items that measure the sedative effects of alcohol, i.e., bored, general prostration, concentration trouble, quailed, sleepy, gloomy, dull feeling in the head, hard to move, becoming calm, slow thinking, being inactive and feeling tired (16). Each item was supposed to be checked among 10 scores which had "never" representing a score of 0 and "definite" representing a score of 10. The total scores (between 0 to 120) for the stimulative effect were determined by adding up each score for the 12 items. This meant that the higher the scores are, the higher the stimulative effect of drinking is. The sedative effect was determined in the same manner as the stimulative effect.
Visual analogue scale for craving (VAS-C)
VAS-C, which measures the extent to which one craves alcohol, is required of subjects to check how they respond to the 130 mm parallel line marked "never" on the left side and "definite" on the right side. The distance of the checks from the left-sided end of the line is recorded in millimeters and it is considered to reflect the extent of alcohol craving in each subject.
Administration of naltrexone
This study was designed to be a 9-day experiment. All subjects visited our laboratory on the first, second, eighth and ninth experimental days. The 26 subjects were randomly divided into two groups. We used a cross-over design to exclude the effect of the experiment's order. The thirteen subjects of one group (Group 1) were given naltrexone at 10:00 a.m. on only the first (25 mg) and second day (50 mg) and were not given naltrexone on the eighth and ninth day. The thirteen subjects of the other group (Group 2) were not given naltrexone on the first and second day and were given naltrexone at 10:00 a.m. on only the eighth (25 mg) and ninth day (50 mg). To avoid the residual effect of naltrexone and withdrawal symptom of alcohol administration on the first and second day, we made a time interval of 6 days (from second to eighth day).
Measurement of BAES, VAS-C, Blood alcohol concentration (BAC)
On the second and ninth day, the following procedures were proceeded in all 26 subjects (Group 1 and Group 2). All subjects drank soju, Korean distilled spirits in one minute at 12:00 p.m. Each subject drank soju containing 21% alcohol calculated in terms of pure alcohol 0.6 mL/kg. For the experiment, they were prohibited from eating food and drinking water for 2 hr before drinking alcohol, from 10:00 a.m. to 12:00 p.m.
We measured BAES for the stimulative and sedative effects of acute alcohol and VAS-C for craving of all subjects, just before drinking and at 15, 30 and 60 min after the drinking. At the same time, we measured BAC using a breathalyzer (Alco-sensor IV, Intoximeters, Inc., St. Louis, MO, USA).
Group selection by spicy food preference
Twenty-six subjects completed the spicy food preference scale at 9:30 a.m. on the first day. After completion of this 9-day study they were divided into two groups represented by the average scores of the spicy food preference. Thirteen subjects with lower scores were grouped as lesser preference for spicy food, referred to as "LP", while thirteen subjects with higher scores were grouped as strong preference for spicy food, referred to as "SP".
Statistical analysis
The means of age and variables related to alcoholic history between LP and SP were compared by independent t-test. We analyzed the interaction between the changes just before drinking and at 15, 30, and 60 min (4 time blocks) after drinking of the stimulative subscale items of BAES and spicy food preference. This was studied under each condition of the naltrexone condition and non-naltrexone condition (2 drug groups) using repeated measures ANOVA. The sedative subscale items of BAES, VAS-C and BAC were analyzed using the same method. Also, we analyzed the interaction between changes just before drinking and at 15, 30, and 60 min after drinking of the stimulative subscale items of BAES. We sought to determine whether or not naltrexone conditions were analyzed by dividing the subjects into groups that prefer spicy food and that do not prefer spicy food (2 preference groups) using repeated measures ANOVA. The sedative subscale items of BAES, VAS-C and BAC were analyzed using the same method. For the post-verification, a paired t-test was used. We used the Windows SPSS 15.0 with two-sided significance levels less than 0.05.
RESULTS
Comparison of age and variables related to alcoholic history between LP and SP
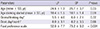
The means of age, the age at which drinking started, the average drinking amount on each drinking day for the last 12 months and the average drinking day per month for the last 12 months did not differ significantly between LP and SP (Table 1).
The stimulative effect of acute alcohol using the stimulative subscale items of BAES
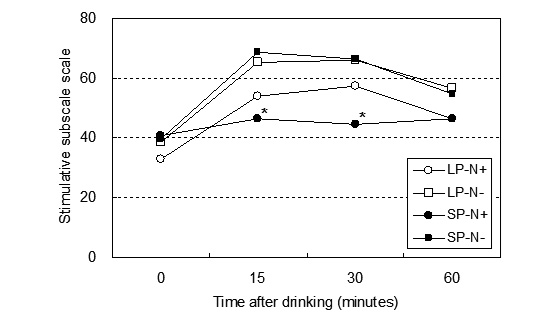
Repeated measures ANOVA (2 preference groups×4 time blocks) on the stimulative subscale of BAES revealed a significant group by block interaction in the naltrexone condition (N+) (df=3, F=8.20, P<0.001), but not in the non-naltrexone condition (N-) (Table 2 and Fig. 1).
Repeated measures ANOVA (2 drug groups×4 time blocks) on the stimulative subscale of BAES revealed a significant group by block interaction in SP (df=3, F=7.91, P<0.001), but not in LP. The paired t-test revealed that significant suppression of the stimulative subscale of BAES was observed at 15 min (df=12, t=-4.31, P<0.001) and 30 min (df=12, t=-4.36, P<0.001) after drinking when N+ was compared with N- in SP (Table 2 and Fig. 1).
The sedative effect of acute alcohol using the sedative subscale items of BAES and the alcohol craving using VAS-C, as well as the BAC
For the sedative subscale of BAES, VAS-C and BAC, repeated measures ANOVA yielded no significant group by block interaction by either spicy food preference or naltrexone administration (Table 2).
DISCUSSION
In this study, we found that acute alcohol effects are not different according to the spicy food preferences without naltrexone administration. There was no difference in the stimulative and sedative effect of alcohol between the group who preferred spicy food and who did not when naltrexone was not given to the subjects. This result contradicts the assumptions of this study. However, after naltrexone was administered, the stimulative alcohol effect was suppressed by naltrexone in SP group, but not in LP group. Results of the present study correspond to the results of our preliminary study which reported that the acute effect of alcohol intake was not different according to spicy food preference, but was more suppressed by naltrexone in those who preferred spicy food (14).
The absence of difference in acute alcohol effects between SP and LP group suggests that acute effect of alcohol does not react with the central opioid system alone but reacts with many nervous systems like dopamine, gamma-aminobutyric acid (GABA), and glutamate. However, given the small number of subjects in this study, it is necessary to pursue this research with more subjects.
Many studies have substantiated the fact that naltrexone is effective in treating alcohol dependence; however it appears that this does not apply to everyone. It has been reported that naltrexone had the effect of preventing the relapse of alcoholism among 70%-75% of the subjects (7, 17). Based on these results, many researchers are recently looking for an efficient subtype of naltrexone. They have substantiated that naltrexone is more effective in circumstances such as the high level of craving for alcohol, poor cognitive function, and a strong family history of alcoholism (18, 19, 20). The results of this study showed that the stimulative effect of acute alcohol administration was suppressed by naltrexone in the spicy food preferring group. In a previous study that investigated the effect of naltrexone on acute alcohol response, naltrexone suppressed the stimulating effect of alcohol, increased the tranquilizing effect and suppressed the craving for it (21). These results imply that naltrexone could prevent a relapse more effectively in those who prefer spicy food, but future studies will be required to ascertain the role of spicy food preferences in the treatment of alcoholics with naltrexone.
In SP group, the sedative effect of acute alcohol administration and the craving for alcohol were not suppressed by naltrexone. Given that the sedative effect of acute alcohol administration was significantly increased at 90 min after drinking in social drinkers (21), the fact that this study was carried out only until 60 min after drinking can be considered its limitation. Moreover, it is difficult to assume the reason for no significant effect on the craving for alcohol, but the individual difference in the craving for alcohol can be one of the possible reasons.
Our results imply that spicy food preferences may be associated with opioid system activation which is blocked by naltrexone, a nonspecific opioid receptor antagonist. Interestingly, it has become known that food preference is related to the pleasure effect gained by food (22). The pleasure effect by food reward system is connected to opioid activity (23). Therefore, an interrelationship between the taste preferences and the alcohol dependence may be possible. The results of previous studies showed that people who have a greater preference for sweetness have a positive family history of alcohol dependence (24, 25). Another study showed that people who are more sensitive to bitterness have more alcohol-related problems and a greater family history of alcohol dependence compared to those who were less sensitive to bitterness (26). According to the results of one study, genes that are related to the bitter-taste receptor revelation are related to alcohol dependence (27).
Our study has several limitations. The biggest limitation is the measuring method for food preference. The FPS was not standardized and its reliability and validity should be verified. Another limitation was the small number of subjects and short measuring time for alcohol effect, especially sedative effect.
However, no studies have been concerned with the relationship among the spicy food preference, the acute effect of alcohol drinking, and naltrexone. Further studies will need to ascertain the relationship between other taste preferences and alcohol's effect, and its implication in the treatment of alcohol dependence. This study is significant in that it is the first to present the relation between the remedy of alcohol dependence and spicy food, in particular, spicy Korean food.


 XML Download
XML Download